This case report focuses on the significance of understanding the patho-physiological changes occurring in the body and timely diagnosis of disease based on presenting symptoms and investigations and formulation of correct homoeopathic therapeutic strategy.
Furthermore, association of extent of damage with consideration of existing comorbidities like hypertension, diabetes, or ischemic heart disease is an important aspect to take into account while managing an acute disease developing during the course of chronic illnesses.
Damage due to these acute insults is much more serious and sudden in preexisting deranged organs. Here, we focus on a 65-year-old hypertensive female brought to the emergency room with acute symptoms of profuse diarrhoea and vomiting leading to severe fluid loss. She was diagnosed as suffering from acute gastroenteritis leading to pre-renal azotemia which needs to be corrected at the earliest by administration of IV fluids. The homeopathic simillimum in correct potency and repetition is needed to prevent further loss of fluids.
KEYWORDS:
Diarrhoea, Pre-renal azotemia, Tubercular Miasm, Podophyllum, James B. Bell, Typhoid fever
INTRODUCTION:
WHO has identified Acute Diarrheal Diseases (ADD) as one of the leading causes of mortality in developing and underdeveloped nations. It is one of the top 10 leading causes of death especially in children. ADD can also adversely affect old aged individuals. They can easily get dehydrated leading to electrolyte imbalance and renal damage.
Old aged individuals are suffering from life style disorders like hypertension and diabetes mellitus. This increases the risk of the target organ damage due to ADD induced hypovolemic AKI (Acute Kidney Injury). Pre-renal azotemia is the condition characterized by abnormally high levels of nitrogen waste products occurring as a result of loss of body fluid commonly seen in cases of severe diarrhoea, vomiting, burns etc., compromising renal plasma flow / blood flow and intra-glomerular hydrostatic pressure which leads to acute kidney damage.
Homoeopathic physicians should formulate the treatment strategy based on pathological expressions. All the investigations and therapeutic processes should be simultaneously executed in order to stabilize the vitals of the patient and correct the dehydration.
Renal insufficiency caused by fluid loss must be corrected by administration of IV fluids along with suitable homoeopathic remedy. Failure to do so may lead to irreversible kidney injury and renal shutdown. Homoeopathic intervention is based on the disease process and expressions, like causation, stool character, color, quantity, and type of evacuations. These are some of the key indicators which can point towards a group of remedies and make the final selection easier and quicker.
The concept of time and pace of disease is the foremost thing which needs to be considered while selecting a remedy as mentioned by Dr. Boger in is Synoptic Key. Each homoeopathic medicine has its own pace of symptom manifestation during drug proving; so it is important that time dimension and pace of disease should match drug pathogenesis pace during the process of cure.
CASE REPORT:
Preliminary data:
Mrs. K. B., Age: 65 years brought to the casualty on 05/12/21 at 10.30 am by her relatives
Chief complaint: K/c/o Hypertension since many years.
| Location | Sensations | Modalities | Concomittant |
| Gastro Intestinal System
since 4 days Stomach/ Rectum Abdomen Rectum Passes 3-4 times a day |
Profuse Diarrhea 3 + Vomiting 3+
Fever Mild Pain Character of stool: Copious+3, Water+3, Greenish+3, Non-offensive, Frequency of urine had reduced considerably and patient was unable to recollect when she passed urine in last 6-8 hrs. Thirst: Increased+3; drinking sips of water with fear of vomiting and diarrhea Weakness3+ Clinical Findings: Pulse: 101/min BP: 110/70 mmHg Per Abdomen: Soft, tenderness present Bowel sounds present |
Vomiting
< Eating or drinking 3+ Fever > after antipyretic Weakness <Diarrhea and Vomitting3+ |
Treatment H/O:
Received antibiotic treatment without relief
- Tab Cifran 500 tds Tab Ornidazole 500 (1-1) 3.Tab Ondem 4mg (1-1)
- Tab Cyclopam (1-1-1) 5. Anti Hypertensive Tab. Telista 20 od
CLINICAL APPROACH:
Patient had acute diarrhoea with copious stool and vomiting which led to severe acute reduction in body fluids leading to decrease in the blood flow to the kidney resulting to renal dysfunction, decrease in the urine output (kidney was trying to compensate the fluid loss by preserving the further loss of sodium and water into the urine).
INVESTIGATIONS:
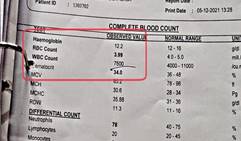
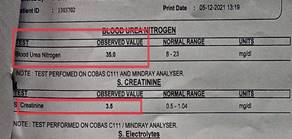
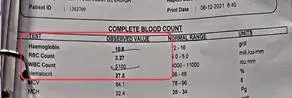
| Figure 1: CBC Date: 05/12/21 | Figure 2: BUN and S. creatinine Dated: 05/12/21 |
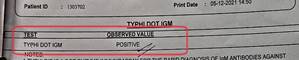
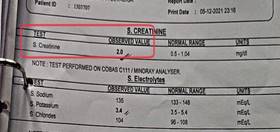
| Figure 3: Typhi DOT IgM Dated: 05/12/21 on the day of visit to the emergency room | Figure 4: S. Creatinine Dated: 05/12/21 at 10:56 pm after the administration of IV fluids and homeopathic similimum |
| Figure 5: CBC dated 06/12/21 |
Interpretation of the Investigations
- Typhi Dot IgM test was positive (Suggesting recent Salmonella infection)
- Blood urea nitrogen and Creatinine levels were high
- Low serum electrolyte levels
- Decrease in the RBC count
Enteric Fever with Predominant Enteritis with Short lasting Fever
Typhoid fever is an intestinal infection caused by Salmonella enterica serotype S. typhi which may present with symptoms such as a high fever, prostration, abdominal pain, diarrhoea or constipation and skin rash.
In this case the patient developed typhoid fever with short lasting fever but severe gastroenteritis compromising renal functions. There is a disappearance of fever due to symptomatic treatment by a general practitioner.
STAGE OF DISEASE (ASSESSMENT OF RENAL COMPROMISE AND ITS STAGES)
RIFLE CRITERIA ARE AS FOLLOWS:
| Risk | Injury | Failure | Loss
(more than 4 weeks with persistent acute renal failure) |
End stage kidney disease
(> 3months of complete loss of kidney function) |
|
| Creatinine | 1.5 fold increase from baseline | 2 fold increase from baseline | 3 fold increase from baseline | ||
| GFR | > 25% increase from baseline | > 50% increase from baseline | > 75% increase from baseline | ||
| Urine output | < 0.5ml/kg/h for 6 hours
|
<0.5ml/kg/h for 12 hours | < 0.3ml/kg/h for 24 hours or anuria for 12 hours |
According to AKIN criteria, increase in the S. Creatinine level to more than 50% of baseline value or presence of oliguria for more than 6 hours is considered as diagnostic criteria for AKI
As per the investigations done on 15/12/21,
| Test value | Baseline value | |
| S. CREATININE: | 3.5 mg/dl | 0.5-1.04 mg/dl |
| BLOOD UREA NITROGEN: | 35 mg/dl | 8-23 mg/dl |
In this case, there is an increase in S. Creatinine to around 3 fold of baseline value with decrease in the urine output and loss of vital fluid in the form of diarrhoea and vomiting. Thus according to RIFLE criteria, these investigations are suggestive of “ACUTE RENAL FAILURE OF PRE-RENAL ORIGIN”
DIAGNOSIS:
Enteric Fever Salmonella Typhi presenting as acute gastroenteritis with pre-renal azotemia with acute kidney injury.
CONVENTIONAL LINE OF TREATMENT/ MANAGEMENT
- Antibiotic treatment should be started as soon as possible in cases of typhoid fever.
- Most effective therapy for patient with acute kidney damage is careful management of fluid balance, which involves thoughtful assessment of hydration, a fluid treatment plan personalized for the specific patient, repeated and frequent reassessment of fluid and electrolyte balance, with appropriate changes in the treatment plan in response to the rapidly changing clinical situation of the patient.
- Patient was already being treated by administration of antibiotics for three consecutive days but patient’s health status was not improving. Instead patient’s health deteriorated further and administration of NSAIDS contributed in causing renal compensation by bringing about reduction of renal blood flow and GFR
- Also, the patient is hypertensive. Hypertension and older age can lead to structural narrowing of the intra-renal arterial and impaired capacity for renal afferent vasodilation.
- All the above factors aggregated are suggestive of Pre-renal azotemia.
HOMOEOPATHIC THERAPEUTIC STRATEGY:
Objective of the treatment:
- Prevention of further fluid loss in the form of vomiting and diarrhoea along with restoration of normal fluid volume.
- To Correct Electrolyte Imbalance.
- To Normalise the serum creatinine level with the help of the correct Homoeopathic remedy and Ancillary/ Auxiliary line of treatment.
- Priority is to normalise the renal function and avoid the need for Dialysis.
Therapeutic approach:
- Stage of disease is reversible pathological change without permanent damage to the nephrons. Based on the above understanding there should be remedy selection which matches the pace of disease and reverse the pathology.
- Concept of susceptibility in such high paced evolving disease is very crucial in order to apply the correct simillimum with correct posology and repetition to reverse the disease phenomenon.
- In such acute debilitating cases, with susceptibility at new ebb and the critical state threatening every moment to extinguish the life force within, it will be sheer folly to expect the simillimum unaided to save the life. It will have to be reinforced by other appropriate measures like (i) Replacement therapy and (ii) Anti-bacterial therapy which doesn’t mean the failure of law of similars but in fact demonstrates its judicious application in practice and a comprehensive appreciation of the clinical situation that prevails. (Dr M.L. Dhawale, Principles & Practice of Homeopathy)
Therapeutic strategy:
| Date | Problem
Definition |
Problem Resolution
(Methods and Techniques) Process End Point |
Precautions and Dangers | |
| 5/12/21 | Acute Diarrhoea with copious stool and vomiting leads to severe volume depletion leading to AKI as seen as
S. Creatinine 3.5 mg/dl (up to 1 mg/dl) S.BUN 35mg/dl |
1. To restore the volume depletion and dehydration by administration of intravenous fluids thus improving renal perfusion.
(IV Fluid administration is guided by S. electrolyte levels) 2. Prevention of further fluid loss in the form of vomiting and diarrhoea by giving the right similimum based on the Prescriptive totality. 3. To Monitor Input and Output in order to titrate the intravenous fluid and avoid fluid overload. 4.To Correct borderline Hyponatremia in order to avoid deterioration in level of consciousness. 5. To Normalise the serum creatinine level with the help of the correct homoeopathic remedy and IV fluids. (Note: Serum creatinine can decline even on IV fluids but Diarrhoea and vomiting will not stop with IV Fluids, it requires correct similimum). S. Creatinine should be checked after 6-8 hrs. to document the trend of decline or ise. |
1. Urine output initiates will indicate restoration of Blood Volume.
2.When vomiting and diarrhoea stops and there is reduction in the frequency of repetition of Homoeopathic remedy Stop IV fluids if dehydration, S.Electrolytes and S.Creatinine are corrected. |
1. When IV fluids are administered in cases of low urine output and azotemia, it may result in cardiac overload and pulmonary edema.
(Need proper assessment of input output charting and timely chest examination for developing Basal Crepts on auscultation). 2. Remedy response should be analysed every 1 hourly. If remedy fails to register it needs to be changed immediately based on emerging totality to avoid further fluid loss. Avoid over correction which may lead to Hypernatremia, Fluid overload and Cerebral edema. Avoid potassium rich food, as in acute damage to the kidneys. Potassium excretion is decreased and hence serum potassium level is high which may have adverse effect on heart If Creatinine levels fails to reduce than there should be nephrological reference taken and They usually start Diuretic therapy in low doses along IV fluid infusion under supervision so that the patient starts urinating. If creatiine doesn’t improve then dialysis will be required. |
Boger’s Prescriptive Approach
- Boger’s methodology is a complete therapeutic strategy mainly based on the pathogenetic totality. Based on the pathogenetic totality obtained, appropriate rubrics are found to form a contour of the disease picture.
- Boger’s approach is adapted in cases which are rich in particulars with marked modalities and concomitants, pathological generals, and clinical symptoms, objective and pathological symptoms, cases without many mental symptoms.
- Similar is the scenario in this case, where the seat of the disease is pathological evolving with rapid pace and needs to be assessed at earliest based on the acute totality which again needs to be based on the knowledge of the cause of the disease, without it, the choice of similimum cannot be made with safety
Principle of Boger’s approach:
- The cause of the disease
- Seat of the disease or what is the pathology of the disease
- Modalities
- Sensations
- Mental generals
Based on the Boger’s approach, we consider the following acute totality for the selection of similimum:
Acute totality:
- Inflammation: intestines (enteritis)
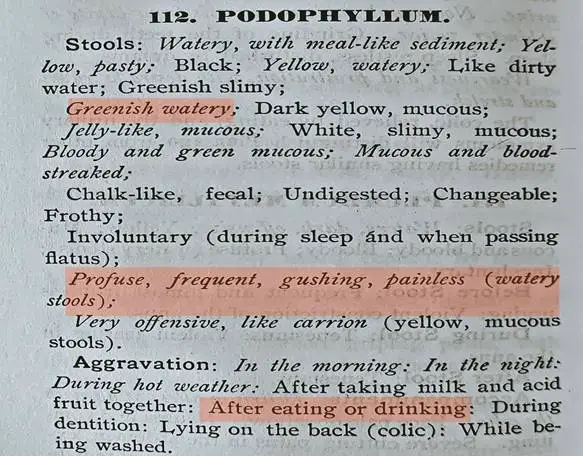
- Diarrhoea: Copious+3
- Diarrhoea: greenish+3
- Diarrhoea: watery+3
- Diarrhoea: Painless+3
- Diarrhoea: Frequent+2
- Thirst+3: for sips of water throughout the day
HOMOEOPATHIC THERAPEUTICS OF DIARRHOEA BY JAMES BELL
It is the type of clinical repertories which emphasis mainly the loose evacuations
It was not originally intended to be based solely on the diarrhoea but it was constructed on the basis of types of stool, aggravating and ameliorating factors, causation and concomitant symptoms
Construction of Bell’s diarrhoea is based on:
- Hahnemann’s chronic diseases
- Jahr’s new manual
- Boenninghausen’s therapeutic pocket book etc
The book explains the therapeutic use of 141 drugs in cases of diarrhoea
REPERTORIZATION USING HOMOEOPATHIC THERAPEUTICS OF DIARRHOEA BY JAMES BELL (HOMEPATH APP)
REPERTORIZATION USING BOERICKE’S REPERTORY (HOMEPATH APP)
ACUTE REMEDY DIFFERENTIATION:
| Podophyllum | Phosphorus | Arsenic | |
| Causation | Over-straining
Summer (diarrhoea) |
Strong odour
Loss of fluids Tobacco |
Eating fruits
Poor diet Chills Decayed food |
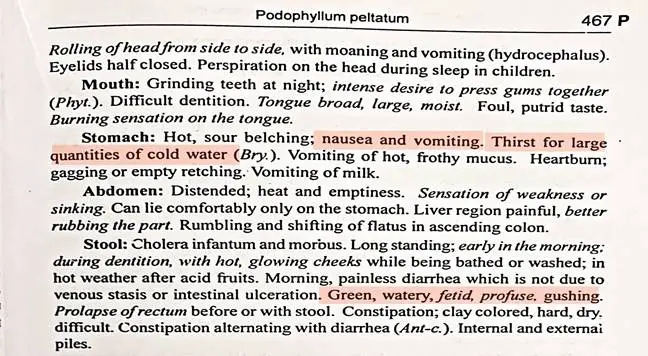
| Stool | Morning diarrhoea
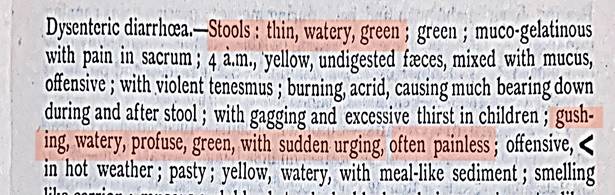
Diarrhoea immediately after eating or drinking Stool:thin, watery, green, with sudden urging and often painless Extreme exhaustion after stool |
Diarrhoea in great quantity like water from a hydrant
Painless, involuntary Undigested faeces greenish, grey watery with whitish yellow cheesy masses Pain in stomach chiefly after meal |
Violent diarrhoea with frequent evacuations
Involuntary painless diarrhoea of yellowish, greenish, brownish or blackish foetid evacuations Evacuations of undigested substances |
| Vomiting | Nausea distressing and extreme with attempts to vomit
Vomiting of milk, of food Vomiting <eating |
Nausea with violent hunger and thirst >eating or drinking water
Vomiting of food <evening
|
Frequent and excessive nausea, sometimes even rising to throat
Vomiting after having drunk or eaten |
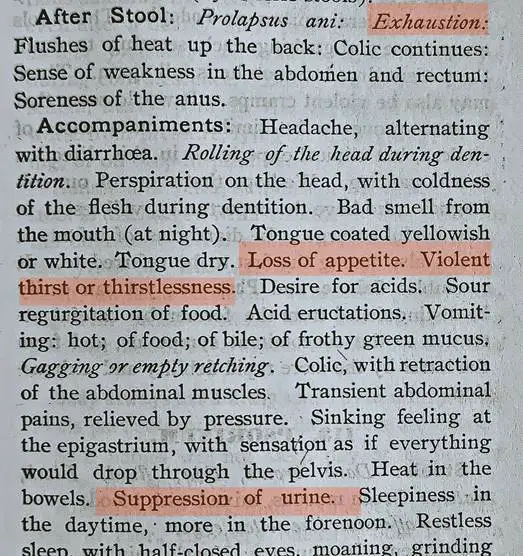
| Thirst | Thirst for large quantity of cold water | Thirst for refreshing drinks, for cold water | Burning thirst |
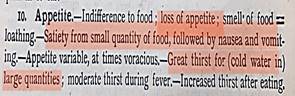
| Appetite | Indifference to food
Loss of appetite Satiety from small quantity of food followed by nausea and vomiting |
Violent hunger
Hungry soon after eating |
Want of appetite and hunger
Continual craving |
| Modalities | <eating, drinking, acid fruits
> lying on abdomen |
<warm food or drink
>cold food |
<cold food or drink
>warmth in general, warm food |
FINAL ACUTE REMEDY:
PODOPHYLLUM
The Homoeopathic Therapeutics of Diarrhoea by James B. Bell
BOERICKE’S MATERIA MEDICA
MATERIA MEDICA BY CLARKE
Posology:
HIGH/ 200th Potency
- Suitableness of a medicine for any given case of disease does not depend on its accurate homoeopathic selection alone, but likewise on the dose as well.
- As mentioned by Dr. M. L. Dhawale in his Principles and Practice of Homeopathy, high potency can be administered in case of acute illness with changes in vital organs and in cases with extremely close correspondence of the remedy to the picture as presented by the patient.
- Under these circumstances, the remedy is repeated frequently till a definite response is seen.
- In this case, focus is on stopping the symptoms of diarrhea and vomiting and preventing the disease from further progression. Here, there is acute onset, severe intensity and rapid progression of disease and thus the dose of the disease should be high enough to overpower the effect of disease but not very high to worsen the patient’s health status, and thus 200th potency was selected. Also the antibiotic treatment was given to the patient but there was no change in the presenting symptoms and thus there was no suppression of the disease which indicates that the patient’s susceptibility is high and thus high potency in correct repetition should be given to affect the cure
Repetition of dose:
- In acute cases, the action of the remedy is known to exhaust early and therefore, frequent repetition is indicated. As the response is obtained, the frequency is cut down progressively so that the dose tapers gradually
- Premature cessation of the remedy is known to promote a relapse
- Similar is done in this case, as there is presence of acute progressive disease, the simillimum is repeated at every 15 minutes first and as soon as the response is seen, as soon as the patient’s condition is getting better, the repetition is reduced to every 2 hourly.
- Also, it is mentioned in aphorism 248, of Organon of medicine that, in acute cases, repetition of dose every 2-6 hours and in very urgent cases, every hour or oftener is admissible.
- Doses can be repeated frequently in acute cases even if medicine is so highly potentized with ever so many succussions.
- So, it was done in this case, simillimum in high potency was first repeated every 15 minutes for 24 hours and once the patient’s state of health was showing improvement, the repetition was reduced to 2 hourly.
1st Prescription at 2PM :
Rx Podophyllum 200 Every 15 minutes
Auxiliary line of treatment:
- Avoid potassium rich food, as in acute damage to the kidneys potassium excretion is decreased and hence serum potassium level is high which may have adverse effect on heart
- Minimise protein intake
- Avoid high sodium diet
- Fluid intake needs to be regulated on the basis of urinary output and other water loss from diarrhoea or vomiting
- Consume a minimum of 600-1000kcal
- Generally 35-50 kcal per kg body weight should be consumed to maintain positive nitrogen balance
FOLLOWUP AND OUTCOMES:
Followup criteria:
- Stool (frequency, consistency)
- Nausea
- Vomiting
- Fever
- Appetite
Follow up:
| Date | General wellbeing | Appetite/ thirst | Stool frequency | INPUT | OUTPUT | O/E | ACTION | |
| 5/12/21
3.30 pm |
Weakness because of diarrhoea | Appetite decreased | 2 episodes of diarrhoea since admission
Stool: watery, greenish, dark and profuse |
Rx
Podophyllum 200 Every 15 minutes |
||||
| 5/12/21 | Patient is comfortable | Diarrhoea frequency and quantity is much better
Consistency is still watery but better than earlier |
IV: 3500ml
Oral: 600ml
Total intake: 4100ml |
Urine: 450ml
Stool: 7 times |
Podophyllum 200 4 pills every 15 minutes
|
|||
| 6/12/21
early morning |
Patient is better and stable | Frequency of stool: twice throughout the night
Consistency is still the same |
Urine passed 3-4 times | BP: 120/80 mmHg | ||||
| 06/12/21
4.00pm |
Pt. is overall better | Frequency of diarrhoea is reduced
Consistency is same: green, watery |
10RL – 10DS – 10DNS
Over 6 hourly each |
BP: 120/80mmHg | Podophyllum 200
4 pills every 15 minutes |
|||
| 6/12/21
11.40pm |
Pt. is overall better | Tolerated soft diet (Khichdi) | One episode of loose motion since morning | IVF 6 hourly each | Urine output:
1100ml |
Podophyllum 200
5 pills every 2 hourly
|
||
| 7/12/21 | Pt is overall
better |
Podophyllum 200
5 pills every 8 hrly |
||||||
| 14/12/21 | CHRONIC TOTALITY:
– Fear of darkness+2 – Fear of heights – Anxiety in closed space – Aversion to noise – Desire fish+2 – Desire warm food+2 – Desire chinese+2 – Aversion to milk |
Pulsatilla 200 1P HS
SL 30 qds x 1 week. |
||||||
Overview of the Remedy response:
- Patient was brought to the emergency room by her relatives on 05/12/21 at 10.30am. On the basis of presenting symptoms, seat of the disease and investigations with high S. Cr & BUN value, Podophyllum was prescribed on the same day with the repetition at every 15 minutes till the patient’s health started to improve and then the repetition was reduced to every 2 hour. Serum Creatinine and BUN values were brought back to the normal range within 48 hours and the patient was discharged on morning of 07/12/21
Follow up investigations:
| 05/12/21
(1:15 pm) |
05/12/21 (10:56 pm) | 06/12/21 (08:11 am) | 06/12/21 (1:25pm) | |
| HB | 12.2g/dl | 10.6 | ||
| RBC | 3.99 mil/cumm | 3.27 mil/cumm | ||
| WBC | 7500/cumm | 5100/cumm | ||
| S. SODIUM | 132mEq/L | 135 mEq/L | ||
| S. CREATININE | 3.5 mg/dl | 2.0 mg/dl | 1.1 mg/dl | |
| BUN | 35mg/dl | 20.9 mg/dl | ||
| TyphiDOT IgM | Positive |
Figure 6: Graph representing the Serum Creatinine levels before and after treatment.
Discussion and Observation during treatment:
- Recovery always depends on the prior state of health, severity of illness and process of care.
- The course of disease, with progression or improvement, consequently represents both nature and extent of injury and repair, the associated comorbidities, and the management.
- AKI due to volume depletion and loss is often treated by Modern Medicine by providing Proper Anti- Diarrheal, Anti- Emetics and Antibiotics. These sets of Medicines are replaced by single Homoeopathic Medicine which is based on symptom similarity.
- Acute renal failure may result in complete recovery in some patients and partial recovery in others. Basis for the complete recovery is the absence of AKI criteria which is mainly focused on the S. Cr levels, GFR and urine output of the patient
- According to the studies and researches conducted over the years, AKI major cases occur as a result of pre-renal cause and takes around 7 days for complete recovery with appropriate treatment.
- In this case, after administration of homoeopathic simillimum along with IV infusion, the decline in the serum creatinine level was seen in 6 hours from the initiation of the treatment. Complete normalisation of S. Creatinine was seen in less than 24 hrs.
CONCLUSION:
- This case demonstrates the role of homoeopathic medicines in acute debilitating cases and the efficacy of homoeopathic management in the cases not responding to the primary antibiotic treatment.
- Understanding the pathology of the disease is as important as understanding the symptomatic evolution of the case.
- Assessment of susceptibility and miasmatic evolution of disease is important for correct prescription.
- Selection of correct potency and adequate repetition of the dose is as important as selection of simillimum for any given case and any lapse in above can lead to ill management of the case.
ACKNOWLEDGEMENT:
I would like to thank Dr Mohanbhai Patel, Chairman, The Homeopathic Education Society, Mumbai. Dr Asmita Parikh, The General Secretary, The Homeopathic Education society, Mumbai. Dr Parizad Damania, Principal, Smt Chandaben Mohanbhai Patel Homeopathic Medical College, Vile Parle west, Mumbai. Dr Asha Chaudhari, Intern, Smt Chandaben Mohanbhai Patel Homeopathic Medical College, Vile Parle west, Mumbai.
REFERENCE:
- Dennis L. Kasper, Stephan L. Hauser, J. L. Jameson, Anthony S. Fauci, Dan L. Longo, Joseph Loscalzo. Harrison’s principle of internal medicine, 19th edition, volume 2, McGraw Hill Education, Part-13, p. 1799-1800
- John Henry Clarke. A dictionary of practical materia medica. Volume III, B. Jain Publishers, p. 869-871
- Boericke W. Boericke’s new manual of homoeopathic materia medica with repertory. 3rd revised and augmented edition based on 9th edition. B. Jain publishers. p. 466-7
- James B. Bell. The Homoeopathic Therapeutics of Diarrhoea: Dysentery, Cholera morbus, Cholera infantum and all other loose evacuations of bowels. P. 168-170, 209-12
- WHO newsroom. Diarrhoeal disease, fact sheet. Published on 2nd May 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease
- Shreya Gupta, Dr. Ashish Ranjan. TyphiDot test, Overview. Lab tests. Available from: https://www.1mg.com/labs/test/typhi-dot-2292
- John P. Cunha. Acute Kidney Failure: Facts you should know about acute kidney failure. Available from: https://www.emedicinehealth.com/acute_kidney_failure/article_em.htm
- Colin Tidy, Dr. John Kox. Article on Typhoid and paratyphoid fever. Available from: https://patient.info/travel-and-vaccinations/typhoid-and-paratyphoid-fever-leaflet#:~:text=It%20is%20possible%20to%20have,only%20carriers%20of%20these%20infections.
- Sapna M. Repertorization methods by CM Boger. From Articles on Homoeopathic . Repertory. Available from: https://www.homeobook.com/repertorization-methods-by-cm-boger/
- M. L. Dhawale. Principle and practice of Homoeopathy, Part-1. 2004. Published by Dr. M. L. Dhawale memorial trust. p. 281
- M. L. Dhawale. Principle and practice of Homeopathy. Part-1. 2004. Published by Dr. M. L. Dhawale memorial trust. p. 254
- Samuel Hahnemann, Dr, William Boericke. 6th edition of organon of medicine. Aph. 248. p. 273
- Samuel Hahnemann, Dr. William Boericke. 6th edition of Organon of Medicine. Aph. 275, 276 and 279. p. 298-300 and p. 302
- Samuel Hahnemann, Dr, William Boericke. 6th edition of organon of medicine. Footnote 133 to Aphorism 247. p. 272-73



