
The patient is a 94 -year-old woman suffering from later stage dementia and Alzheimer’s Disease. She requires 24 hour assistance. She has trouble recalling events, faces and names of even family members and can often misplace words or slip into other languages.
For the patient‘s consultation, the I spoke to one of her daughters, who, along with her brothers, are caring for her. Before the consultation, background information was shared with the practitioner, and I was made aware that there would be an interpreter for the reason that the patient does not speak too clearly, nor English very well.
Note: I was able to directly speak to the patient for the last 30 minutes of the consultation, the entire time she was cooking and moving about the kitchen. Multiple times, her daughter had to get up to aid her mother.
When the patient finally did sit down, her gaze was distant – she made an off hand comment about the trees out the window, wistfully blowing in the wind. It was making her sad. The patient’s daughter and her aunt have commented that she has always been dreamy, but recently has been especially so and distant.
The patient has been through a tumultuous life, to say the least. When she was 9 years old, she was taken from her family [sold by her mother]. There is anger when talking of her mother.
She was in an abusive relationship with her husband. She has expressed that she has never felt ‘free’ that she feels ‘caged’ and never had a chance to be herself. The patient’s daughter mentions that she often denied things, it was a way to cope. It has been suggested that she dissociates, which is common in people who suffer trauma /PTSD.
There is extreme irritability and mood swings. Anger brought on when she does not get her way or there is a lot going on, -noise and people- she feels out of the loop. The patient can scream in anger, and the patient’s daughter mentions that once recently she hit and would strike.
She is also very sensitive. She is sensitive to the emotions of others. If people argue in front of her, she will easily get agitated, and it’s not uncommon for her to take their fighting personally as something she has done wrong.
There is a great fear of the dark. Sundowning. As the sun goes down, symptoms become worse. She becomes agitated. The sadness is worse. There is difficulty sleeping, and resistance to retire when the time comes or bed. The patient can be tired and nodding off, but will refuse to go to bed. She may fight.
She misses her family greatly. Since she was 9, she’s never been back to visit. The patient cares for her family very much, but she herself feels as if her family (childhood) never cared for her, abandoned her and so feels unloved.
The patient’s daughter often tries to remind the patient that she is very loved, but she does not always “hear it”. She has another daughter, who is estranged from the family, which the patient refuses to talk about. When the patient’s daughter mentions her sister’s name, the patient cannot recall the name or the person behind it.
There are feelings of worthlessness, like she did not do enough. That she did not do her job as a mother/wife.
OBJECTIVE FINDINGS
Sundowning is a common symptom seen in Alzheimers and Dementia, along with increased agitation and irritability and confusion. These symptoms are usually brought on around dusk or when the sun goes down and can continue into the night.
INITIAL ASSESSMENT
For a 94 year old woman, she is active, and determined in her endeavors. She was focused on cooking and asked for help when she needed it. But the irritability and obstinacy were also visible, as she did refuse to take a seat for the consultation, and she was not able to focus and have a conversation.
For this case, I was not able to communicate with the patient directly, because of the language barrier and also because of the nature of her illness. She was responsive or prudent to the conversation seldom during the interview, and her daughter/caretaker provided the bulk of the background and context. Asking the patient direct questions, translating, and then relaying, and then providing any extra information she felt was necessary to share.
For this reason, it was imperative to take the daughter’s theorizing of the patient’s emotions, feelings and reactions with a grain of salt. As useful as they are because they are so close and that is one of the primary caretakers, for the mental and emotional aspects, assumptions may have been made to fill in parts of the patient’s story which were unknown.
As such, when taking the case and looking at the mental and emotional complaints, I did my best to get the general idea of the feeling or theme, and look for a homeopathic medicine that had these same themes.
In terms of the physical/objective symptoms experienced, a lot of the complaints of the patient do seem like symptoms of dementia /alzheimers. I am definitely dealing with a progressive disease. Considering the patient’s age and current status, I would say this is a palliative case.
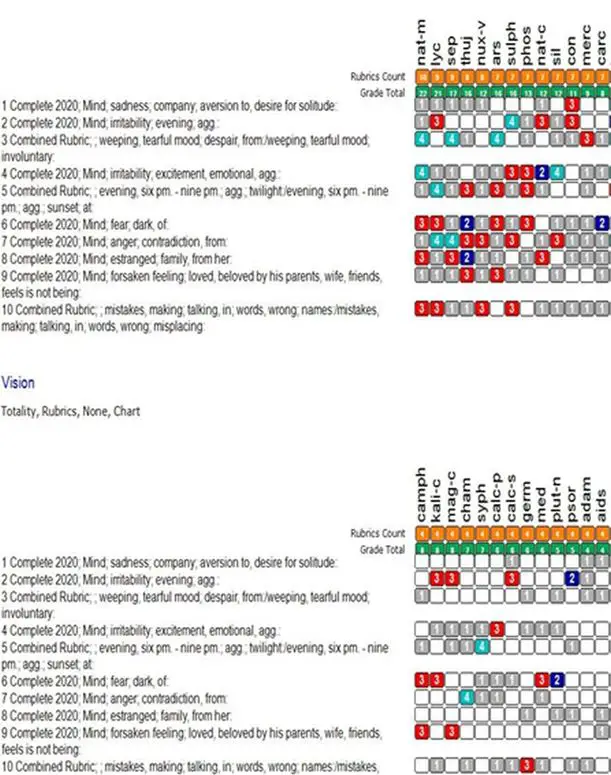
Rubrics & Repertorization
- Mind; sadness, company, aversion to, desire for solitude (57)
- Mind; irritability, restless (42)
- Combine rubric: Mind; weeping, tearful, mood, despair, from/ weeping, tearful mood, involuntary (61)
- Mind; irritability, excitement, emotional, agg (94)
- Combined rubric: Generalities; evening, six pm – nine pm, agg, twilight/ evening, six pm – 9 pm, agg, sunset at (75)
- Mind; fear, dark of (126)
- Mind; anger, contradiction from (84)
- Mind; estranged, family, from her (62)
- Mind; forsaken feeling, loved, beloved by his parents, wife, friends, feels is not being (67)
- Combined rubric: Mind; mistakes, making, talking, in words wrong names/ mistakes, making, talking, in words, wrong, misplacing (102)
Remedy Differential
| Sx | Nat-M | Nat-C | Mag-C |
| Sadness w aversion to company/ consolation | Yes, consolation from others agg her troubles.
(Allens Encyclopedia) |
Sadness (Phatak)
|
|
| Irritability worse in the evening |
|
Fretful, worse in the evening (Allens Encyclopedia) | Irritable (Phatak)
Sx’s worse at night (Lippe) Very ill-humored at 7 P.M., everything is disagreeable, Very fretful in the evening (Allens Encyclopedia) |
| Involuntary, hysterical
weeping Despairing |
Marked disposition to weep; sad weeping mood
She was involuntarily obliged to weep (Allens Encyclopedia) |
Hysterical,
(CD) Sad, melancholy w inclination to weep. (Allens Encyclopedia) |
Anxiety and tearfulness (Boenninghausen) |
| Emotions felt in the stomach | |||
| Emotional excitement aggravates; Irritates | So much excited by the slightest cause (Allens
Encyclopedia) |
Mental distress and shock/ vexation agg
(Boenninghausen). |
|
| Worse in the evening/ sundown/ twilight before dusk | |||
| Great fear of the dark | |||
| Anger from contradiction | Become violent and passionate at every trifle
(Allens Encyclopedia) |
He is angry, and inclined to fight and strike, and cannot
tolerate contradiction, in the forenoon (Allens Encyclopedia) |
|
| Feels estranged from her family | Very fretful and discontented with the whole world
(Allens Encyclopedia) |
||
| Feels forsaken/ unloved by her family | Aversion to mankind and society ( Boericke)
Dejection (CD) |
Yes | |
| Makes mistakes in talking/ calling names | Easily makes mistakes in talkingDulness and loss of
thought, with sleeping; worse from 3 to 7 P.M.,1. |
He easily makes mistakes in writing
(Allens Encyclopedia) Mental weakness (Boericke) |
Dazed feeling (Phatak) |
| (Allens Encyclopedia)
|
Difficulty of comprehension, which is unnatural to him
when in health; imbecility, or weakness of intellect. (CD) |
||
| Other Sx | |||
| Etiologies | Vexation; disappointment; fright; | Vexation; mental distress; shocks. | |
| Depressed and full of grief
Always in his thoughts to seek for past unpleasant occurrences, in order to think them over, making himself morbid When alone. she becomes uneasy about herself, and must weep She felt almost as if losing her reason Very weak memory; everything remains in his mind like a dream Religious melancholy |
Anxiety
Hasty restlessness He cannot think easily; the power of concentration fails He stares without thought, as if stunned by a blow Inquietude, with fits of anguish,
|
Very sensitive
Sleeplessness at night from restless anxiety Constipation For several nights was unable to fall asleep for a long time on account of anxiety; Better in the evening,
|
Remedy Choice
a) My choice of remedy is: Nat-c
My reasoning for wanting to give Natrum carbonicum over the other remedies:
- The mental and emotional symptoms of Nat-c are more in line with this patient than that of the other remedies. The sadness, despondency, and some irritability.
- The feelings of unworthiness are strongest in this remedy -unworthy of love (not because of looks as in Nat-m)
- The disposition to weep, that can be hysterical weeping, < from consolation.
- The feeling of being estranged and forsaken is strong in this remedy. History of it in the patient (Forsaken/sold by her mother)
- There is a level of extreme anxiousness in this remedy. In this patient, she appears worried, and confused, leading to restlessness and anxiety and fearfulness in the patient.
- The sensitivity of the remedy matches the patient’s; the sensitivity to noise is apparent. Natrum being a mineral remedy, I think may do well for her complaint having to do with her self-worth, identity, the organization of her home and family and relations (or disorganization of it).
- Natrum remedies are sensitive remedies, and include the theme of grief, which is characteristic to this case.
- The remedy is about the formation and maintenance of relationships, which is also characteristic to the case, since most of her relationships now are strained, which is a stressor on the patient.
The disease is on the mental sphere. Some of it is emotional. Most symptoms had to do with the sensorium. And then the other half of the symptoms were mental traits. I feel like a lot of what I’m dealing with in this case is underlying experiences in her history that are still affecting her negatively today.
Past traumas, self-limiting beliefs (that she is unloved, that she cannot express herself, that she is the issue). However, looking at the nature of the illness and the age of my patient and the progression of the illness (the Alzheimer’s/ Chief Complaint), and the profundity of which her history runs, I believe a high potency is required. But because of the state of my patient, being so very fragile and old, a lower potency would be best suited. I would like to start at a 12c.
I communicated to the patient’s relatives the treatment plan, and provided them with written instructions as to how to prepare and administer the remedy, including the remedy name, potency and frequency of dosing. The treatment was to take a Nat-c 12c dissolved in 4oz of water, stirred. Take a sip as the remedy. Discard the rest. Repeat as necessary. Stir in increments of 5 stirs of 5 seconds, increasing the number each time you take the remedy.
In conjunction with the remedy prescription, general lifestyle observations were communicated to the patient’s daughter, with the intention to live a hygienic lifestyle, to support the healing abilities of the remedy as well as to support the patient in her day to day.
These recommendations were;
- Continue with the doctor monitoring the Alzheimers.
- Short walks to keep active and combat the restlessness.
- Looking over the diet, to ensure that the patient is getting all essential nutrients. – Continued support and love from her family.
The patient was prescribed the remedy of Natrum carbonicum in 12c, taken 3 times a week, on November 11th.
The first follow-up was conducted on December 20th.
The patient looks much happier. Is smiling, much more engaged and focused. She has new dolls and is introducing them to the practitioner. The practitioner asks her about the dolls, what she likes about them and their names. The answers are not always clear, but the patient is very present.
The patient was a little restless with her sleep after leaving her primary care home the first time after starting the remedy, but the next time, the patient slept well. Is sleeping through the night, without waking which is unusual for them.
There was agitation and irritability, even violent anger, where the patient would strike at those around her if angered before taking the remedy. Very emotional, sad and would cry. This has improved much. There is still some obstinacy and resistance when being told what to do.
In general, the patient is more alert, remembering names and the people around her. The sundowning is much improved, and the incontinence has lessened.
It has not been too long and progress is slowly being made, it is decided to continue treatment as is.
A second follow-up was conducted on January 16th.
There is some grumpiness and irritability, and the patient does not articulate her desires sometimes. Though the mood has generally been good. Only when she is moving from one location to another to stay with different relatives does she become irritable.
This may be expected in someone with dementia or Alzheimers. The idea that a constant change in surroundings and environment, including caretakers, whether they be family or not can be suspected to cause some stress, which it temporarily does.
Her sleep is starting to become restless again, and is refusing to sleep. It is difficult to get her down to sleep sometimes. There is sleepiness during the day. The patient is dozing off during the meeting. The sundowning specifically, is not an issue.
It is felt by the patient’s daughter that the patient has hit a bit of a plateau. Symptoms are not worsening, progress is slowing. The patient has been on a 12c for a long time, to incite the remedy to continue acting, and since the symptom picture has not changed, the decision is made to increase the potency to 30c. Taken 3 days a week, in water.
A third follow up was conducted on February 7th.
There was a lot to go through during this follow-up. After taking the remedy the week after the previous follow up, the patient was very irritable. It did not seem as if that was getting better. The mood swings are faster, whereas before there may have been a progression to anger.
The following week, was very slow. The third week, there was improvements.
There is still resistance to go to sleep, but sleep is deep and she typically stays asleep in the night. The mood of the patient is generally better, more present and responsive. But not as talkative.
After more clarification, it was discovered that the patient had increased the frequency of dosing, as well as the potency. The potency went from 12 to 30c, and posology from 3x/week to 5-6x/week. This is basically giving the patient double the dose that she had previously been taking.
It is believed the aggravation followed by the lull after the second follow-up, was perhaps caused by this shock to the system, of the remedy being repeated so frequently and in stronger potency.
However, the patient has gotten back on track on their own and is doing much better than when the patient had made the follow-up. As such, it is decided to proceed without change. Natrum carb. 30c, 5x/week. The patient’s daughter is advised that should the patient aggravate again, to skip a dose. If the aggravations continue, to discontinue the remedy and contact the homeopath.
Prognosis:
I believe this is a case of palliation, when considering the age and progression of the disease in the patient. I believe it will be very necessary to remain in close contact with the patient and their caretakers to monitor any changes in the system or the symptom picture, to ensure we can give the patient the best care and comfort.
It is not expected that the case will change much, however, I believe with homeopathy, the quality of this patient’s life can be improved, and she can regain some autonomy, and ease any discomfort.



Sir, how long was this patient with constipation, prior to neuro. symptoms.