First Published October 8, 2021 Case Report
https://doi.org/10.1177/09727531211046370
Received: January 29, 2021; August 04, 2021; Accepted: August 04, 2021
https://doi.org/10.1177/09727531211046370
Elena Rudakova1, Seema Mahesh2, George Vithoulkas3, 4
1 Clinic of Nadezhda Kubasheva, Moscow, Russia
2 School of Medicine, Taylor’s University, Subang Jaya, Selangor, Malaysia
3 Department of Homeopathy, University of the Aegean, Mytilene, Greece
4 International Academy of Classical Homeopathy, Alonissos, Greece
Corresponding Author:
Seema Mahesh, School of Medicine, Taylor’s University, No 1 Jalan Taylors, Subang Jaya, Selangor 47500, Malaysia. E-mail: [email protected]
https://creativecommons.org/licenses/by-nc/4.0/
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 License (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access page (https://us.sagepub.com/en-us/nam/open-access-at-sage).
Abstract
Background: Syringomyelia (SM) with Chiari malformation is a rare disease with an unpredictable course. Surgery and other interventions help reduce the severity of symptoms, but over 50% patients require re-operation. Auto-resolution is rare in this type of SM, and most cases progress to complications, which may amount to a great burden.
Case presentation: We present a case of SM with Arnold-Chiari malformation type 1 in a 54-year-old Russian woman who was treated with individualized classical homeopathy for over eight years with remarkable improvement in the clinical signs and symptoms of the condition and comorbidities. On MRI, the syrinx completely resolved, which further confirmed the benefit of this therapy.
Conclusion: This case of SM with Arnold-Chiari malformation type 1 seemed to benefit from individualized classical homeopathy. Scientific investigation into an individualized classical homeopathic approach towards SM is necessary to establish its relevance in this condition.
Keywords
Syringomyelia, Arnold-Chiari malformation, Homeopathy
Introduction
Syringomyelia (SM) is a rare, progressive disease of the spinal cord and it presents with mild to severe neurological complaints, with the characteristic intramedullary cyst,1 occurring mostly from underlying causes such as Chiari malformations (CMs).1 CM incidence is approximately 3–8/100,000, with 62% to 80% exhibiting SM,2 and it shows a predilection to certain geographic locations such as Russia.34 Over 50% of the cases are because of Arnold-Chiari malformation type 1, characterized by herniation of cerebellar tonsils through the foramen magnum, followed by trauma-related incidence (25% of cases), the other types being rarer.15
Many theories were proposed to explain the dynamics behind the development of SM, including the three popular theories of Gardner, Williams, and Oldfield.1 The common vein running through these theories is a disturbance in the circulation of cerebrospinal fluid (CSF), resulting from an aberrant resorption, or a mechanical block to circulation, or disorder of spinal cord mobility.1 SM is classified into communicating, noncommunicating, atrophic, and neoplastic types.
This classification helps decide whether shunting, surgery, or conservative treatment is the best option.6 The understanding of SM pathophysiology remains patchy, which makes its diagnosis and treatment a challenge.7 The diagnosis of SM is made by the appreciation of the fluid-filled cavity in the spinal cord related to CSF circulation disturbance, cord tethering, or an intramedullary tumour.7
The symptoms result from herniation of cerebellar tonsils or the compression of nerves. The most common symptoms in SM with CM are headache, dizziness, insomnia, weakness in the upper extremities, neck pain, numbness and tingling in the extremities, and other neurological symptoms.8 The severity depends on the size and duration of the syrinx.
Rapidly progressing cases show more severe symptoms than cases that progress slowly over many years.4 Management is conservative when neurological symptoms are absent or mild. However, most patients exhibit disease progression with conservative treatment.1
When the symptoms are severe, surgery/shunting/cordectomy/cellular neuro-construction may be offered to the patient, depending on the underlying cause.1 Stabilization of the neurological symptoms and improvement in the general condition are the aims of treatment.2 Surgery is effective in most cases, but over 50% of patients require re-operation at some point.1 Auto-resolution of SM is rarely reported, and sometimes the auto-resolution is not associated with any difference in clinical symptoms.9
We present a rare case of SM with Arnold Chiari malformation type 1 that progressed considerably until the application of classical homeopathic treatment, and regressed under this therapy over the years. A benefit was also seen in the comorbidities. The literature did not yield any other similar case where SM benefited from homeopathy.
Case Presentation
The patient, a Russian woman, medical doctor (ultrasonologist), was 54 years old when she presented for a homeopathic consultation in June 2012. The diagnosis was made in 2006 using an MRI, but she was not given any medication or therapy.
Presenting Complaints
The patient had severe neurological complaints at the time of homeopathic consultation, including pain, burning, and tingling in the dorsum of hands; sharp pains in the first metacarpophalangeal joints; and coldness of the hands. She dropped things suddenly and could not feel how they fell out of her hands. There was pain under the right scapula, in the lumbar and sacral regions, and in her feet. She experienced incontinence of urine when laughing or coughing and reported a pulsating noise in the head.
Other Complaints
Other complaints include deep bleeding cracks in the patient’s fingertips every winter; flushes of heat, disturbing her sleep; dryness in the vagina; epigastric and umbilical region pain with bloated feeling; and deep acne on the face.
History of Presenting Complaints
In 1995, the patient developed vertigo and pain in the hands. She also developed tingling and burning in linear areas in the upper arms, forearms, and dorsum of the hands. Pain in the first her metacarpophalangeal joints increased so much that sometimes she was unable to move the ultrasound probe.
She started dropping things suddenly with insensibility. An MRI in 2006 led to the diagnosis of SM. The neurologist told her to avoid activities such as lifting weights and abdominal crunches, but no therapy/medication was given. She stopped visiting a chiropractor. Follow-up MRIs were performed occasionally.
Past Medical History
The patient suffered hepatitis at the age of three years, had recurrent tonsillitis and occasional gastric pains in childhood, and later developed recurrent tracheitis with high fevers, which continued to occur at intervals at the time of consultation. She was treated mostly with antibiotics for these infections.
At 20 years of age, a gastroscopy revealed no gastritis but an increased motility of the stomach. At the age of 46 years, she was treated with lithotripsy for left renal colic. At 52, she had pneumonia and was given antibiotics. She still suffered occasional flu with high fever. She had pain in the sacral region since she was 34 years old and was visiting a chiropractor for this issue. She had acne since puberty.
Obstetrics and Gynecological History
The patient attained menarche at the age of 13 years. She had two children without event. She underwent electrocoagulation for erosion of cervix at the age of 22 years and laser treatment for leukoplakia of cervix at 45 years.
Since April 2011, she had menopausal symptoms, and a cytological examination of the va-gina showed atrophy of the mucosa. She applied estrogen cream as recommended by the gynecologist but stopped doing it as she developed swelling in the breasts.
Family History
The patient’s father had hypertension and died from rupture of abdominal aortic aneurism at the age of 82 years. Her mother had brain stroke at the age of 65 years, hypertension and vascular dementia. She died at the age of 76 years.

Figure 1. First MRI film in 2006 at Diagnosis of Syringomyelia.
Source:
Diagnosis
The patient was diagnosed as having SM with Arnold-Chiari malformation type 1 (ICD10: G95.0).10
MRI: Cervical and Upper Thoracic Spine on February 15, 2006 (Figure 1)
There is a hydromyelic cavity in the spinal cord extending from the level of C3 to T1 vertebra. The maximum diameter of the cavity is 5 mm. The spinal cord below this level has normal diameter and structure. The vertebral body height is normal, and there are no focal lesions.
There is straightening of cervical lordosis with formation of pathological kyphosis. There is decreased intensity of signal from the intervertebral discs of the cervical spine (evidence of dehydration).
There are dorsal central disc protrusions, up to 3 mm in size, with mild intervertebral foraminal narrowing at the levels of C4–C5 and C5–C6. There is circumferential disc hernia (4 mm dorsally) with signs of intervertebral foraminal narrowing on both sides (mostly right) at the C6–C7 level.
There is descent of cerebellar tonsils below the foramen magnum (an MRI of the brain is recommended).
Conclusion
Hydromyelia at the level of C3–T1. Osteochondrosis of the cervical and upper thoracic spine. Disc hernia at C6–C7.
MRI: Brain and Intracranial Arteries on March 15, 2006
Midline structures are not displaced. The size of the ventricles is normal. There is mild asymmetry of the lateral ventricles (Sinister > Dexter). There are no focal lesions in the brain. Subarachnoid spaces are not widened. The size of the hypophysis is normal.
The stem structures are within normal limits. The cerebellar tonsils extend 5 mm below the Chamberlain line. The paranasal sinuses are filled with air. MR angiography of the intracranial arteries did not show any evidence of occlusion or aneurism of arteriovenous malformations.
Conclusion
There are no focal lesions in the brain matter.
A repeat MRI in July 2008 showed progression of the disease.
MRI: Brain and Cervical Spine on July 22, 2008
The MRI of the brain shows a single, small (up to 3 mm) hyperintense lesion in the white matter of the left frontal lobe near the anterior horn of the lateral ventricle. A second small lesion is at the border between cortex and white matter in the left cerebellar hemisphere.
No other space-occupying lesions or sites of pathological MR-signal are identified. There is widening of perivascular Virchow-Robin spaces. Midline structures are not displaced. The ventricles are of normal position, shape, and size. The lateral ventricles are asymmetrical (Sinister > Dexter).
The basal cisterns are normal. The external subarachnoid space is uneven in width along the convex surface of the cerebral hemisphere; it is slightly dilated in the frontal-parietal areas and normal in other areas. There is ectopia of cerebellar tonsils, not more than 6 mm to the posterior parts of the foramen magnum. The paranasal sinuses are filled with air.
MR angiography of the brain vessels shows no pathological tortuosity, deformities, or dilatations of the arteries, and the vessel lumens are homogenous.
Conclusion Arnold-Chiari Malformation Type I.
Signs of Vascular Encephalopathy
MRI of the cervical spine showed that the syringomyelial cyst found in previous investigations is now extending from the level of C3 to the upper part of the T3 vertebral body. The shape and structure of the cyst (consisting of several confluent cysts with septa) are the same as a previous investigation on December 5, 2006.
The maximum diameter is up to 7 mm at the level of the C7 vertebra. The contour of the cyst at the border with the normal part of the spinal cord is “sharp” – a variant of a cavity with low pressure. The haemangioma at the posterior part of the C7 vertebra is the same in size and shape. Signs of osteochondrosis at the level of C4–C7 vertebrae with maximal pathological changes (posterior disc hernia) at the level of C6–C7 vertebrae.
Conclusion
SM at the level of C3–T3 vertebrae. Osteochondrosis of the cervical spine. Haemangioma of C7 vertebra.
Differential Diagnosis
SM may be confused with neuropathic disorders, such as diabetic neuropathy, and other more common neurological disorders, such as Guillain-Barré syndrome, amyotrophic lateral sclerosis, and multiple sclerosis.11 The diagnosis was confirmed on an MRI of the brain and spinal cord.
Homeopathic Consultation
The patient sought a homeopathic consultation on June 24, 2012. Her neurological symptoms had escalated to the list mentioned earlier. She also had menopausal symptoms and dermatitis. Homeopathic prescriptions consider the totality of symptoms and not just those of SM.
This extends to the patient’s mental/emotional suffering. A detailed history revealed that she suffered repeated events causing grief in the past. She experienced tremendous fear that something bad would happen to her family and they would die.
She dreaded phone calls anticipating bad news. She had sudden episodes of fear, thinking she lost something, such as the keys to her car. She checked and rechecked if she closed the doors and the taps.
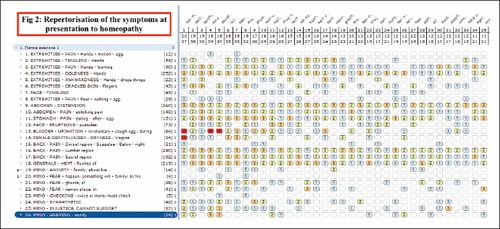
Figure 2. Repertorisation of the Symptoms at Presentation to Homeopathy.
Source:
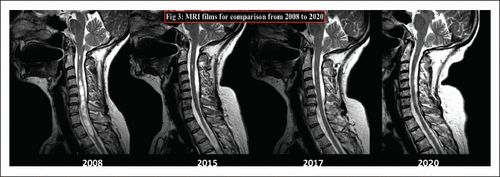
Figure 3. MRI Films for Comparison From 2008 to 2020.
Source:
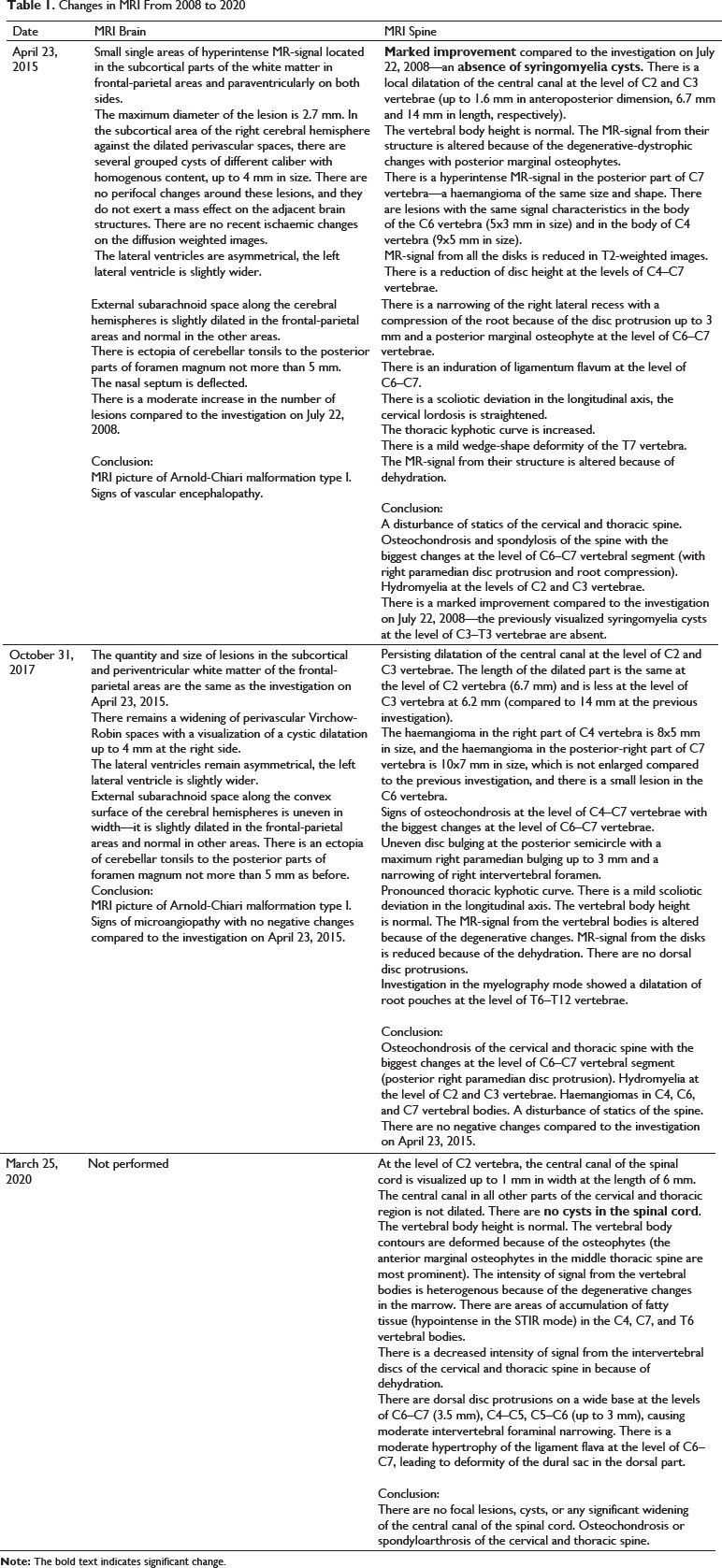
Table 1. Changes in MRI From 2008 to 2020
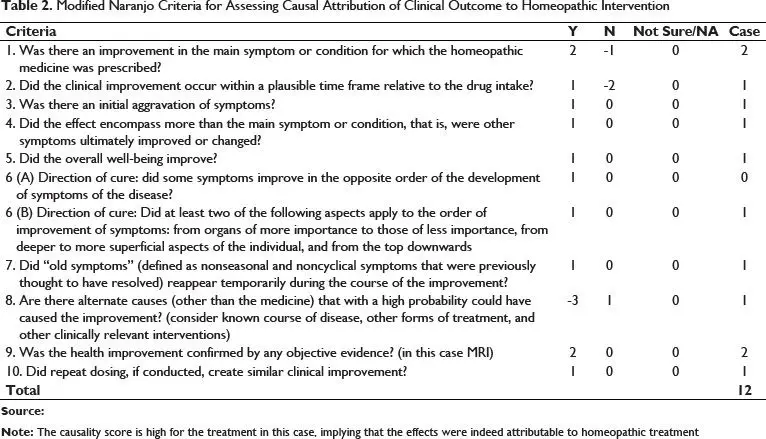
Table 2. Modified Naranjo Criteria for Assessing Causal Attribution of Clinical Outcome to Homeopathic Intervention
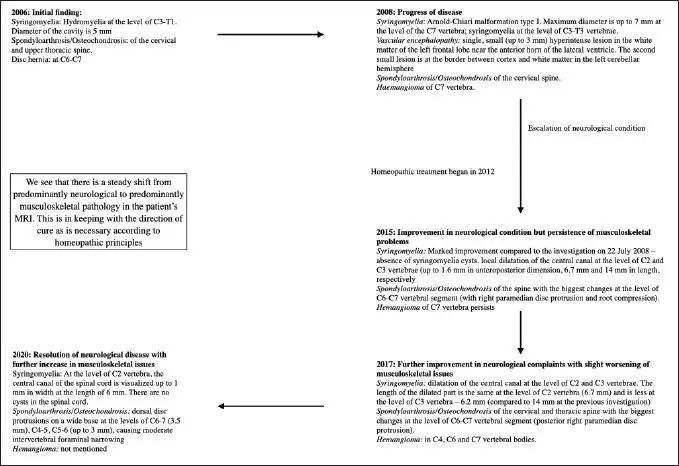
Figure 4. Direction of Cure as Seen in the MRI Reports.
Source:
This specific kind of anxiety and memory loss, along with the history of grief with the physical problems in the nervous system, indicated the homeopathic remedy Causticum hahnemanni (Figure 2).12
Prescription
Causticum 30 CH, One Dose
The rationale behind prescribing Causticum is that the primary pathology in a patient requiring causticum is prolonged grief, bringing down the immune system. A patient in such a condition exhibits absentmindedness and nervousness.
Causticum also has this symptom of having extreme intolerance to injustice from being sympathetic. Further, the cracking of skin and coldness of hands are a part of its proving. The symptom of involuntary urination on coughing is a hallmark of causticum monograph.
Follow Up
After the remedy, pain in the patient’s hands with tingling and burning sensations increased for a period of time (what is termed “therapeutic aggravation” in homeopathy), but the hands became warmer and she sometimes felt heat in her hands. The flushes of heat increased for a period time. Her energy level became better. Her mood improved, and her anxiety diminished.
This case had a long follow up of eight years with constant ups and downs. She received Causticum in different potencies from time to time whenever the symptoms worsened, with good effects most of the time. She also received Causticum for acute episodes, such as trigeminal neuralgia.
Few other remedies were given when she had acute inflammatory diseases, such as common cold, acute otitis media, respiratory infection, and intestinal infection. She was given Mercurius solubilis, Arsenicum album, Graphites, Eupatorium perfoliatum, and Gelsimium sempervirens for these. The otitis did not respond to Graphites, and she used antibiotic ear drops and steroids.
She experienced multiple traumas and fractures during these eight years, despite there being no obvious deficits in her balance, and was given Rhus toxicodendron, Ruta graveolens, and Arnica montana as required. She also received nonsteroidal anti-inflammatory drugs (NSAIDs) for the traumas.
There was once a severe pain in the sacral region that extended to the hip, thigh, and knee. She was then given meloxicam (NSAID) and injections of vitamins B1, B6, and B12. These treatments given interspersed with her main complaints relieved the incidental episodes.
However, the mainstay of her treatment was Causticum, and it nearly always relieved her core symptoms. This is typical in a chronic running case with classical homeopathic treatment, that there may arise need for different remedies during the acute diseases but they may need repetition of the same remedy for chronic condition after such episodes for the case to proceed in the right direction. The relapses were progressively milder over the years until they significantly improved at the last follow-up on October 8, 2020. The patient’s report at the last follow-up is detailed further.
She stopped dropping things and the pain in her hands reduced. She worked more freely. The tingling, burning, and coldness in the hands were gone, and the deep cracks on the fingers disappeared. The acne was less severe.
The anxiety about family was less intense. She did not recheck as frequently. The paresthesia in the calves, which she had experienced since May 2019, had decreased for several days after the last remedy, but relapsed after one week.
The dryness in the eyes that had appeared occasionally since March 2014 persisted. The flushes of heat persisted. Sleep remained poor, waking three to four times during the night, but she fell asleep easier.
Her acute inflammatory conditions over the years became milder than before her starting homeopathy. When asked to repeat the brain MRI for final analysis, the patient refused because she was severely affected by the procedure and, in her own words, “I am healthy, young and beautiful and I will never ever have to do MRI again.”
The changes in the MRI are presented in Figure 3 and Table 1. Notably, the syrinx cavity increased in size from 2006 to 2008, regressed progressively after the commencement of homeopathic treatment, with a complete obliteration of the cavity in the latest MRI of March 2020.
Discussion
In this case of SM with CM type 1, classical individualized homeopathy was beneficial—as appreciated on the MRI—and complete resolution of the syrinx was evident. The clinical signs and symptoms of SM improved along with the crippling anxiety that she suffered. There was also remarkable improvement in her memory, dermatitis, and acne. The frequent infections with high fever also became milder after the treatment.
The causality score on modified Naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention was 12 (Table 2).
The Levels of Health theory13 explains that a patient born with a higher “level of health” generally has a good prognosis despite dire diagnoses. This theory provides tangible methods to categorize a patient’s level of health.
Despite having a chronic neurological condition, our patient generated high fevers during acute episodes, an indication that she was of higher health level and good prognosis. Accordingly, deep positive changes were appreciated in the follow-ups, and she proceeded in the right direction according to homeopathic laws (Figure 4).
She proceeded from a deeper pathology involving the spinal cord (nervous system) to a predominantly vertebral pathology (musculoskeletal system), namely, from SM to spondyloarthrosis. While this may still continue to disturb the patient and require treatment, the limitation is much more superficial.
This effect was demonstrated in other cases with serious pathology, with concomitant ability to induce high fever during acute infections.14 However, such response may not be expected in all cases.
The homeopathic remedy Causticum hahnemanni is indicated in deep neurological conditions, anxiety, depression, and memory issues.12 Classical homeopathy previously exhibited clinical effects in deep pathologies,14 but the effects of Causticum are limited in the published literature.
The limitation here was the inability to demonstrate any pharmacological effect of the remedy because homeopathy does not act on the matter but on the energy fields of the organism,15 a perspective not yet experimentally demonstrated. There is also a remote possibility of auto resolution, as seen in rare cases of SM with CM,9 which was unlikely because our case was on a progressive pathological path at the time of homeopathic consultation.
Conclusion
This case of SM with Arnold-Chiari malformation type I benefited from individualized classical homeopathy, as seen on MRI reports and appreciated in clinical signs and symptoms. There is a need to scientifically investigate the individualized approach to SM cases.
Statement of Ethics
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Authors’ Contributions
Elena Rudakova was the primary physician who treated the patient and who obtained and analyzed the data for the study. Seema Mahesh analyzed the data, wrote the manuscript, and obtained the references. George Vithoulkas was the guide, final approver, and guarantor of the work. All authors have read and approved the final version of the manuscript.
Acknowledgements
The authors are thankful to Aishwarya Madhusudhan for the technical support.
Notes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iD
Seema Mahesh https://orcid.org/0000-0002-4765-5595
https://journals.sagepub.com/doi/full/10.1177/09727531211046370
References
| 1. | Klimov, VS, Gulay, YS, Evsyukov, AV et al. Syringosubarachnoid shunting in treatment of syringomyelia: A literature review and a clinical case report. Zh Vopr Neirokhir Im N N Burdenko 2017; 81(3): 58–65. Google Scholar | Crossref | Medline |
| 2. | Zuev, AA, Pedyash, NV, Epifanov, DS et al. Results of surgical treatment of syringomyelia associated with Chiari 1 malformation. An analysis of 125 cases. Zh Vopr Neirokhir Im N N Burdenko 2016; 80(1): 27–34. Google Scholar | Crossref | Medline |
| 3. | Borisova, N, Valikova, I, Kutchaeva, G. Syringomyelia. Moscow: Meditcina 1989: 5–150. Google Scholar |
| 4. | Bogdanov, E, Mendelevich, E. Syrinx size and duration of symptoms predict the pace of progressive myelopathy: Retrospective analysis of 103 unoperated cases with craniocervical junction malformations and syringomyelia. Clin Neurol Neurosurg 2002; 104(2): 90–97. Google Scholar | Crossref | Medline |
| 5. | Ślusarz, K, Wierzbicki, K, Adamczyk-Sowa, M. Shoulder pain as one of the symptoms of syringomyelia. J. Educ. Health 2019; 9(9) 748–761. Google Scholar |
| 6. | Milhorat, TH. Classification of syringomyelia. Neurosurg Focus 2000 March; 8(3): 1. Google Scholar | Crossref |
| 7. | Klekamp, J. How should syringomyelia be defined and diagnosed? World Neurosurg 2018 March; 111: e729–e45. Google Scholar | Crossref | Medline |
| 8. | Mueller, DM, Oro’, JJ. Prospective analysis of presenting symptoms among 265 patients with radiographie evidence of chiari malformation type I with or without syringomyelia. J Am Acad Nurse Pract 2004; 16(3): 134–138. Google Scholar | Crossref | Medline |
| 9. | Yuan, C, Yao, Q, Zhang, C et al. Spontaneous resolution of syringomyelia with a 16-year serial magnetic resonance imaging follow-Up: A case report and literature review. World Neurosurg 2019 October; 130: 432–438. Google Scholar | Crossref | Medline |
| 10. | ICD-10:, World Health Organization. International statistical classification of diseases and related health problems: Tenth revision, 2nd ed. Geneva. World Health Organization, 2004. Google Scholar |
| 11. | Al-Shatoury, HAH, Galhom, AA, Luzzio, C. Syringomyelia differential diagnoses. In: Selim R. Benbadis and Francisco Talavera (eds.), Syringomyelia. NewYork: WebMD LLC, 2017. Google Scholar |
| 12. | Vithoulkas, G. Materia medica viva Alonissos. Greece: International Academy of Classical Homeopathy, 2001. Google Scholar |
| 13. | Vithoulkas, G. Levels of health (3rd revised edition) Alonissos. Greece: International Academy of Classical Homeopathy, 2019. Google Scholar |
| 14. | Mahesh, S, Mallappa, M, Vithoulkas, G. Embryonal carcinoma with immature teratoma: A homeopathic case report. Complement Med Res 2018; 25(2): 117–121. Google Scholar | Crossref | Medline |
| 15. | Vithoulkas, G, Berghian-Grosan, C. The spin of electrons and the proof for the action of homeopathic remedies. J Med Life 2020 July–September; 13(3): 278–282. Google Scholar | Medline |
View Abstract
SAGE Recommends