
Keywords: COVID-19, SARS-CoV-2, hemorrhagic syndrome, case report, homeopathic therapy
BACKGROUND
Since the report of pandemic outbreak in December 2019, the virus SARS-CoV-2 has infected over 100 million people across the globe and caused death of over two million people, largely affecting the older population and people with co-morbidities like diabetes, hypertension, chronic obstructive pulmonary disease and others.1
The on-going novel infection COVID-19 – as named by WHO, has been reported to produce mild clinical symptoms like fever, cough, myalgia, dyspnea to severe complications like acute respiratory distress syndrome, coagulopathy and septic shock.2
The conventional treatment guidelines set forth are ever-changing, especially with the emergence of new strains of the virus and thereby no clinically approved therapeutics have surfaced so far. Based on the conjecture of viral invasion in the host cells, ACE2 receptor blockers are used to prevent viral entry whereas a group of antiviral drugs like Favipiravir, Remdesivir, Lopinavir, Ritonavir, Chloroquine, Ribavirin and others are administered targeting the viral replication in the host cells.3
In addition to the above mentioned symptoms of the COVID-19 infection, there are evidences for the development of pulmonary thrombosis resulting in thrombotic events such as venous thromboembolism, immuno-thrombosis and disseminated intravascular coagulation4; this led the conventional medical professionals to administering anticoagulant drugs mandatorily for any hospitalized patients with COVID-19 infection, irrespective of a first-rate evidence of clinical thrombosis.5 Consequently, applying anticoagulant strategy for both therapeutic and prophylactic reasons, the cases documented under bleeding complications escalated and eventually led to death.6–9
We present a similar case report of post-acute COVID-19 infection complicated with hemorrhagic syndrome due to overdose of anticoagulants and treated with individualized classical homeopathic therapy.
A 69-year aged male patient, hospitalized for COVID-19 infection was on anti-viral drugs, along with oral anticoagulants. The patient additionally suffered from co-morbidities like 2nd degree hypertension, duodenal ulcer and prostate adenoma. Chronically managed under conventional treatment and during homeopathic treatment in the hospital set-up, the patient was on antipyretics and antibiotics.
CASE REPORT
69 year old, male
Homeopathic intervention: 04.05.2021
Background
Co-morbidities – 2nd degree hypertension, duodenal ulcer, prostate adenoma.
Patient was treated at the hospital from 19.04.2021 to 28.04.2021 for covid19 infection (PCR test for SARS CoV2 +ve on 09/04/2021), non-hospital bilateral poly-segmental pneumonia, 2nd degree respiratory failure. After discharge from the hospital, on the recommendation of the attending physician, he received Xarelto 10Mg/day daily (Rivaroxabanum, High Selective Direct Factor Xa Inhibitor) without coagulogram control.
On the 4th day, internal bleeding developed: melena, hematuria and hemoptysis.
On 02.05.2021, he was hospitalized in the surgery department of the city hospital with a diagnosis of “internal bleeding, bleeding stomach ulcer, 3rd degree hemorrhagic shock, post-hemorrhagic anemia, bleeding from the bladder.”
General blood test 02.05.21:
Hemoglobin 83 g / l (N – 120 g/l), erythrocytes – 3.4 -1012 / l (N?), leukocytes – 29.9 – 109 / l (N 4-9 – 109/l, ESR – 34 mm / h (N – 2-12), band neutrophils 34% (N < 5), segmented 47%, Eosinophils – 3%, Lymphocytes – 14%, Monocytes – 2%.
Urine analysis 02.05.2021: Erythrocytes cover the entire field of view, urine is cloudy, brown in color, protein, sugar is not detected.
Conventional Treatment: Antibiotics, hemostatic therapy (tranexanoic acid, dicinone), intravenous infusion (trisol, reosorbilact).
Despite the therapy, the patient’s condition worsened, and the relatives were warned by the medical staff about the possibility of patient’s death.
Homeopathic intervention: 04.05.2021
State on 04.05.2021: extreme weakness, nausea, severe shortness of breath, pallor.
O2 saturation: 89-93, temperature: 37.7oC.
Hemodynamics unstable, blood pressure – 80/50 mm Hg, pulse – fast and difficult to palpate, melena continues, urine is brown and scanty (daily urine output 200 ml).
Patient was half asleep, eyes closed and swollen ankle.
Speaks with difficulty and again falls into a stuporous state, but extremely irritated from noise or when they turn him in bed.
Prescription: Considering the etiology (massive blood loss) and the patient’s condition, CHINA 200C was prescribed – in solution every three hours.
FOLLOW UPS:
| DATE | FOLLOW UP | PRESCRIPTION |
| 05.05.2021 | Condition better.
Temperature- 38.6 C BP 110/70 mm/Hg Hemodynamics stable Weakness reduced, clear consciousness, bleeding stopped, shortness of breath persists. The patient was transferred from the surgical department to the pulmonology department due to bilateral pneumonia and received infusion therapy, along with antipyretics and antibiotics, which could not be canceled despite requests from relatives. |
Continue |
| 06.05.2021 | Condition worse.
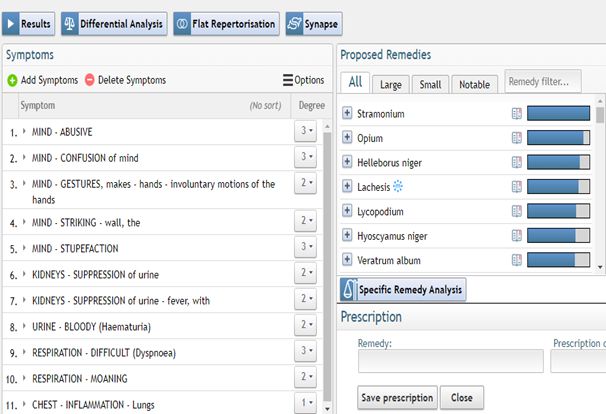
Temperature: 38.5 C O2 saturation: 90-93, oxygen concentrator was required. Ultrasound of the abdominal organs did not reveal any pathological changes. Ultrasound of the chest organs – consolidation of the lower parts of the lungs, effusion into the right pleural cavity. Lies with eyes closed, moaning while breathing, confused consciousness, involuntary movements of the fingers of the left hand, while the right one hits the wall or makes wavy movements, grimaces with his lips and face, shakes his head from side to side. Face is red. Sometimes opens his eyes, responding to the voice, with a frightened look, shouts out curses, threatens, jumps out of bed, cannot tolerate heat. Requires constant presence of his daughter. He does not know where he is, he does not remember his name. The daily urine volume is reduced (300 ml), the urine is dark, cloudy. |
STRAMONIUM 200 CH – every three hours.
(See repertorization 1.) |
| 07.05.2021 | Condition improved.
O2 saturation: 92-95 Less confusion, communicates adequately. Breathing better. He became calmer, there is no aggression or excitement. No obsessive movements. Since he was in the intensive care unit, he received antibiotics, antipyretics, diuretics, antifungals, antacids and infusion therapy. The urine has become lighter, there is less blood and its volume is larger. |
Continue |
| 09.07.2021 | Relapse.
Temperature – 38 C Respiratory rate 28-30/min Heavy breathing, shortness of breath, red face, fingers scratching on the wall, pulling the blanket, waving his hand in the air. He again became aggressive, swears at the medical staff and his daughter who cares for him. Periodically falls into a stupor. Does not tolerate sweet food, requires sour food. |
Stramonium 200 – every three hours |
| 10.05.2021 | Condition improved.
O2 saturation: 95-97 without O2 concentrator. Patient even apologized for his behavior when the nurse made a remark to him. He began to take interest in his wife’s condition, who was also hospitalized with covid19 infection. The urine is light, the volume is sufficient. No shortness of breath. From the intensive care unit, he was shifted to the therapy department. |
Continue |
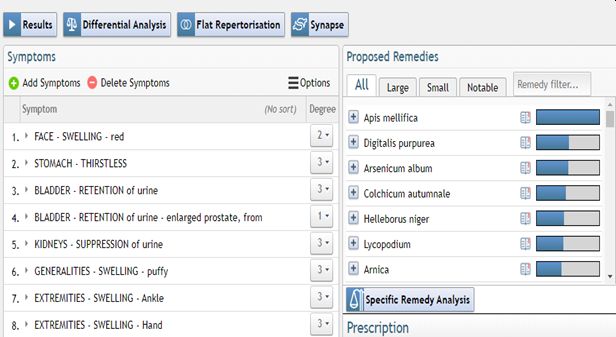
| 11.05.2021 | Against the background of allopathic treatment, anuria occurred after removal of the catheter, there was a question about staging an epi-cystostomy.
Swelling of the hands, ankles and face. Face red. No thirst. Angry and swears. He wants be cooled. |
Apis 200C once.
(See repertorization 2.) The daughter stopped all allopathic treatment on her own. |
| 12.05.2021 | Diuresis resumed, edema is less, the condition is better in all respects.
Appetite increased. Discharged from hospital, home care under the supervision of a family doctor. |
Continue |
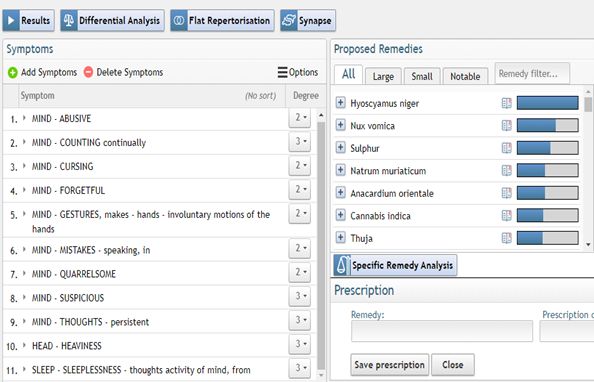
| 19.05.2021 | Relatives note a sharp change in patient’s behavior after being in the hospital. He became suspicious, aggressive, constantly insulting his wife. He began to control the time, constantly monitoring the numbers on the clock. Obsessive. Suffers from obsessive thoughts about work, which is why he suffers from insomnia. Constant uncontrolled movements with the right hand (like a pendulum). Constantly confuses words; implies one meaning but says another word.
Relatives are afraid that he will go crazy, because the brother suffers from schizophrenia from a young age, and his sister had Alzheimer’s disease. His father died of a brain tumor at the age of 56. As a child, he suffered from tics and stuttering after fright. |
Hyoscyamus 200 C single dose
(See repertorization 3.) |
| 22.07.2021 | The mental state has improved, there are no obsessive thoughts, does not confuse words. He became calmer and had a good sleep. There are no obsessive hand movements. There is no heaviness in the head.
In recent weeks, he noted a difficulty in the urine outflow and a bifurcation in the urine stream, which he had several years ago with prostate adenoma, after which he took Tamsulosidum 0.4 mg per day (an alpha 1-adrenergic receptor antagonist). The Patient is on further treatment. |
THUJA 200C one dose |
Repertorization 1 – 06.05.2021
Repertorization 2 – 11.05.2021
Repertorization 3 – 19.05.2021
DISCUSSION
SARS-CoV-2 viral invasion poses a significant threat to its host’s immune system, persistently incapacitating the defence mechanism with low vitality and latent chronic ailments. This subdued state of immune system is further magnified by the massive drug regimen taken conventionally to do away with the infection.
Classical homeopathy is a system of medicine that works by reinforcing the immune system, and in situations like the on-going pandemic when infection becomes severe, homeopathy provides a more specific approach to the condition arresting the process of decline; and the same is being demonstrated in this paper.
The patient was hospitalized for COVID-19 infection and progressed to 2nd degree respiratory failure. After recovery he was advised to continue oral anticoagulants without coagulogram control. During homeopathic intervention, the patient’s hemodynamics were unstable, with extreme weakness and pallor; the remedy China 200C was prescribed based on the pathophysiology of the process of decline – massive blood loss.
Within 24 hours, the patient’s hemodynamics was stable, and his consciousness became clear with an awareness of his surroundings, while formerly he was in a stuporous state. After China 200C controlled the internal bleeding, Stramonium 200C was further prescribed when the patient’s oxygen saturation dropped. After 5days of this remedy, the patient was shifted from ICU to a general ward and was finally discharged from the hospital.
After this what followed was a unique phenomenon in the health status of the patient, which is often overlooked by the conventional school – a predisposition that can get activated as a result of severe immunological challenge and how this is becoming increasingly apparent with chronic sequalae of COVID-19 infection.10–13
As a consequence of this, in our patient the signs of neuropsychological degeneration started manifesting with progressive impairment of behavioral and cognitive functions (see table), owing to the activation of the latent inherited pathology – schizophrenia and Alzheimer’s disease (AD).
This development may also be attributed to neuroinflammation, as the most recent studies have identified an association between the virus and AD resulting from neuro-invasion and are urging for new therapeutic strategies.14–16
At this stage he was prescribed Hyos 200C, the remedy expeditiously halted further neurological degeneration, and brought the patient back to his original health level; the last remedy prescribed was addressing his prostate adenoma, one of his chronic complaints. The patient is still under homeopathic treatment for his chronic ailments, and we expect he will proceed towards general improvement in all his pathologies.
CONCLUSION
The case report presented here is a good example of treating a complicated state of decline in COVID-19 infection and how post-covid activation of chronic issues was handled with individualized classical homeopathic therapy. We need further such instances to strongly establish the efficacy of homeopathy.
REFERENCE
- Coronavirus Disease (COVID-19) Situation Reports. Accessed August 27, 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
- C H, Y W, X L, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (London, England). 2020;395(10223):497-506. doi:10.1016/S0140-6736(20)30183-5
- J M, T M. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021;23(1). doi:10.1208/S12248-020-00532-2
- V C, G S, R R, et al. Anticoagulant treatment in COVID-19: a narrative review. J Thromb Thrombolysis. 2021;51(3):642-648. doi:10.1007/S11239-020-02242-0
- Barnes GD, Burnett A, Allen A, et al. Thromboembolism and anticoagulant therapy during the COVID-19 pandemic: interim clinical guidance from the anticoagulation forum. J Thromb Thrombolysis. 2020;50(1):1. doi:10.1007/S11239-020-02138-Z
- C M, D S, T C, P R, N U. Anticoagulation and In-Hospital Mortality From Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin Appl Thromb Hemost. 2021;27. doi:10.1177/10760296211008999
- Al-Samkari H, Gupta S, Leaf RK, et al. Thrombosis, Bleeding, and the Observational Effect of Early Therapeutic Anticoagulation on Survival in Critically Ill Patients With COVID-19. Ann Intern Med. 2021;174(5):622-632. doi:10.7326/M20-6739
- R P, D C, G P, et al. The hazard of (sub)therapeutic doses of anticoagulants in non-critically ill patients with Covid-19: The Padua province experience. J Thromb Haemost. 2020;18(10):2629-2635. doi:10.1111/JTH.15022
- P L, S G, K M, I V, M Z. Heparin-Induced Thrombocytopenia in COVID-19. J Investig Med high impact case reports. 2020;8. doi:10.1177/2324709620944091
- MT H, D G, E L, D M, R B. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimers Res Ther. 2020;12(1). doi:10.1186/S13195-020-00640-3
- V H, D S, EP D, I P. COVID-19: from an acute to chronic disease? Potential long-term health consequences. Crit Rev Clin Lab Sci. 2021;58(5):297-310. doi:10.1080/10408363.2020.1860895
- PK P, IK S, R B, Y S. Case Report: Dengue Virus-Triggered Parkinsonism in an Adolescent. Am J Trop Med Hyg. 2020;103(2):851-854. doi:10.4269/AJTMH.20-0039
- O M-P, GC R, R P-T, Y R, JM A. Concurrent Guillain-Barré syndrome, transverse myelitis and encephalitis post-Zika: A case report and review of the pathogenic role of multiple arboviral immunity. J Neurol Sci. 2018;395:47-53. doi:10.1016/J.JNS.2018.09.028
- EE B, S K, TK R, BG P, BH M. Anticipating and Mitigating the Impact of the COVID-19 Pandemic on Alzheimer’s Disease and Related Dementias. Am J Geriatr Psychiatry. 2020;28(7):712-721. doi:10.1016/J.JAGP.2020.04.010
- MA R, K I, S R, M A. Neurobiochemical Cross-talk Between COVID-19 and Alzheimer’s Disease. Mol Neurobiol. 2021;58(3):1017-1023. doi:10.1007/S12035-020-02177-W
- AS Z, LS M, T G, S F, DE K, S S. Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review. JAMA Neurol. 2020;77(8):1018-1027. doi:10.1001/JAMANEUROL.2020.2065




Thank you for posting your case, you handled it remarkably! Your feedback is precious.
Thank you, Nataliia. Your case description, inclusion of repertory sheets and analysis are invaluable.