Since the earliest days of Homeopathy, efforts have been made to explain the phenomena of Homeopathy according to the science of the day. (1) Never have these explanations been adequate because our understanding of the subtleties of nature are imperfect. Nevertheless continued attempts to form a physical working model to explain the phenomena of Homeopathy have been made through the years because there is a segment of the Homeopathic community which is not satisfied with just knowing that Homeopathy works (by whatever mechanism), who are more comfortable with physical constructs than theoretical ephemera, and/or who simply like to explore those grey areas of the unknown/unknowable.
This activity is not confined to the field of Homeopathy. In the mid-20th Century, Quantum Physicists, bogged down in their attempts to explain the phenomena of quantum physics through complicated mathematical equations, began to use simple, artificial models called Feynman Diagrams to visualize the events of quantum physics, to explain the results of their experiments, and to predict the existence of yet to be discovered subatomic particles.(2) These diagrams are two dimensional suggestions of the events occurring in the nano-world of quantum physics, not actual renderings of the events. Yet they have served the quantum physics community well through the years in allowing the scientists to more easily comprehend a world they cannot see.
It is with this same intent that the authors would like to introduce the following graphic representation of the workings of Homeopathy – knowing this model is not a picture of the actual events but rather a suggested visualization for study and clarification. To this end, let us consider a potential configuration of this physical model. If we consider health and disease to be a continuum (3), we need a geometric figure which could represent such a continuum.
At first, a line would seem a logical choice since it is the simplest continuous figure. But when we look at life, a straight line seems too static. We know that life involves certain rhythms and fluctuations (circadian rhythms, menstrual periods, sleep/wake cycles, pulses, biorhythms). A straight line seems inadequate for such a dynamic system.
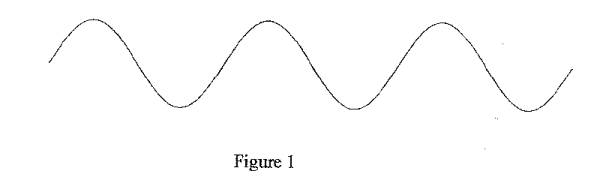
These rhythms seem to suggest a sine wave as the logical representative figure. (Figure 1) Often rhythm and balance are represented using such a wave (as in harmonics, coherent sound waves, etc.). If we believe health is a state of balance and harmony and that life encompasses certain rhythms, then indeed the sine wave seems to be a good choice. Any distunement (disease) imposed on this system would appear as disruptions on this synchronous wave.
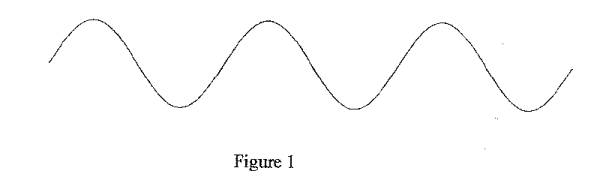
If we accept the synchronous sine wave as the basic representation of the state of the Vital Force in health, we can see that the infinite variation in wave length and amplitude allows for the representation of the unique character of each individual Vital Force. For the sake of developing the concepts of this model, we will let the amplitude of the sine wave represent the vitality/relative health of the individual and the wave length represent the unique character of the individual.
Also for the sake of graphic representation, let us assume that events nearer the base line are more superficial in nature and events nearer the apex of the wave represent deeper, more energetic episodes since they are more divergent from the norm of the baseline.
Thus the unimpinged Vital Force will have a synchronous sine wave whose wave length is of an individual nature and whose amplitude is a function of individual vitality. Disruptions occurring near the base line will be displayed physically as superficial symptoms (either superficial in location or nature). Disruptions nearer the apex will manifest physically as deeper or more pathologic symptoms.
Now consider the nature of chronic disease – the miasms of Hahnemann. We know that the principle miasm is Psora. (4) Psora must be present before the other miasms can manifest. (5) Also consider that the miasms are contagions which act as parasites (1) As living entities (parasitic contagions) they must have their own Vital Forces, and can thus be represented by their own sine waves.
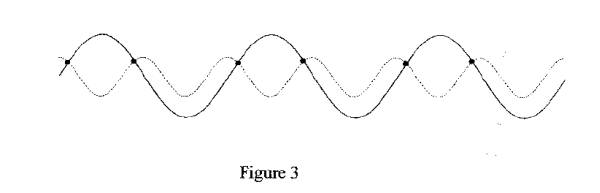
What happens when the synchronous system of the patient is impacted by the synchronous system of the chronic disease miasm? If the miasm is truly a parasitic contagion (6), we will first see Psora attaching to the Vital Force of the patient. This results in a system of two simultaneous sine waves, with points of intersection causing a pattern or resonance and interference unique to the combination and phase of the two sine waves.
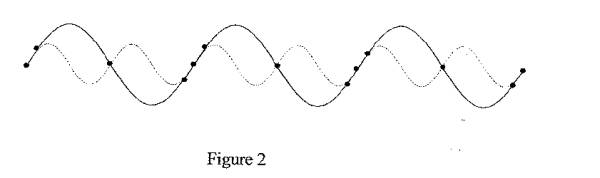
It is at these points of intersection that two changes occur. First, the synchronous wave of the patient’s Vital Force is disrupted (impinged by the miasm) causing symptoms in the patient. The points of intersection are unique to the combination of the patient’s sine wave’s amplitude and wavelength and the phase at which it encountered the impingement of the miasm. (Figures 2 and 3) This allows for the infinite array of symptoms on all levels which we see in patients, even though we only classify and recognize the three classical miasms of Hahnemann.
The second result of this intersection of sine waves is an establishment of contact between the host and parasite. This gives the parasitic miasm a point of attachment from which to derive energy from the host.
As stated earlier, we are assuming that points of intersection closer to the base line result in more superficial symptoms and points of intersection closer to the apex of the waves result in deeper or more pathological symptoms. Using the above model, we can visualize how less vital patients (weaker Vital Forces/lower wave amplitude) will show deeper symptoms – the relative difference between their sine wave amplitude and that of the miasm is small, resulting in points of intersection relatively closer to the apex of the patient’s sine wave. Conversely more vital patients will have a relatively greater distance between the apes of their wave and the apex of the miasm’s wave, resulting in the production of more superficial symptoms.
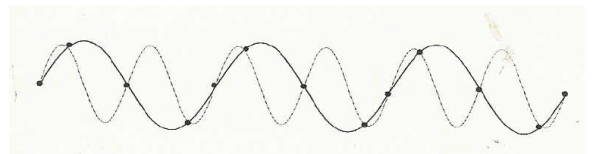
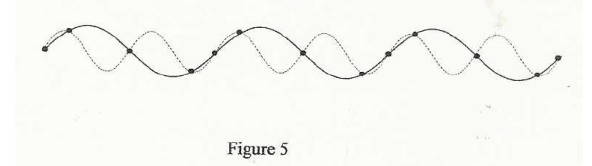
We can also visualize what happens over time as the patient is impinged by the influence of the parasitic miasm. As the parasitic miasm contacts the patient at the intersections of their respective sine waves and derives energy from this contact, we will see either the amplitude of the miasmatic wave increasing as it gets stronger from the patient/host’s energy (Figure 4) or we will see the amplitude of the patient/host’s wave decreasing as it is deprived of energy by the parasite (Figure 5). Either way, there is a decrease in the difference of the amplitudes of the two wave systems, with the result of increased likelihood of points of intersection relatively closer to the apex of the patient’s wave – deepening of the symptoms of the patient with the progress of chronic disease.
Again it is easy to see how this system accounts for the vast array of symptoms we see in clinical practice and for their relative frequency. Mathematical probability for the intersection of the sine wave of the miasm with the patient’s sine wave based on wavelengths and phases will account for the likelihood of common or unique symptoms we see in practice. The higher the mathematical probability for the point of intersection, the more often we will see the symptom which results from that point of intersection/impingement. Conversely, the lower the mathematical probability, the less often we will see a particular point of impingement (symptom). Strange, rare and peculiar symptoms result from lower probability intersections and are thus more statistically significant in matching patient to remedy. (7)
However, we also see common patterns in our patients (constitutional types, miasmatic trends, essences, etc). This can be accounted for graphically by similar wavelengths allowing for close trends of impingement with subtle individual variance. Thus superficially the patients with similar wavelengths will resemble each other because of the similarity in sine waves resulting in similar points of intersection but on closer examination there will be individualizing characteristics from dissimilar points of impingement.
If this graphically represents the influence of the miasm on the patient and the progression of chronic disease in the body, what happens as we treat the patient with the well selected Homeopathic remedy?
Hahnemann says that two similar diseases cannot exist at the same time in the same body, and that the stronger of the two will permanently displace the weaker of the two. (8) In this model, a similar medicinal disease will compete with the miasm at the points of intersection. Since the medicines are chosen based on their ability to cause similar symptoms, we can infer that they impinge the Vital Force at the same points as the miasm. In competitive binding, the object with the stronger affinity for the point will displace or prevent the impingement of the object with the weaker affinity. As the medicine occupies the point of intersection, it will deny the interaction of the miasm with the Vital Force at those common points. This will, in effect, deprive the miasm of its energy source. (6) As with all living organisms, when there is no energy input, viability ceases. As the vitality of the miasm ceases, the likelihood of it reestablishing after the medicinal effects dissipate decreases – it dies from lack of energy.
Since the medicine has a finite life span, it will eventually dissipate and leave the Vital Force without impingement. At this point the sine wave of the Vital Force can and must return to a synchronous state – health.
As the miasm is deprived of its energy source and weaken (or as the Vital Force strengthens because there is no longer an energy drain by the miasm), we see an increasing difference in amplitudes between the sine wave of the miasm and the sine wave of the Vital Force. As this gap increases, we see the points of intersection appearing relatively closer to the base line of the sine wave of the Vital Force (farther from the apex). This results in symptoms becoming more superficial in a display of Hering’s Law.
This also allows for the return of old symptoms as previous points of impingement are passed in the reversal of vitalities. Since the respective wave patterns are the same for the Vital Force and the miasm as the patterns of the past, this shift in amplitudes will cause old symptom patterns/points of impingement to be reestablished temporarily.
The degree to which we see this happen depends on the exactness with which the medicine matches the impingement of the miasm on the Vital Force. If the match is complete, we see a complete competition and removal of the miasm (and a total removal of the symptoms). If the match is only partial, we see a partial removal and weakening of the miasm but a continuation of symptoms from the remaining points of impingement. These then must be addressed with a remedy appropriate for the current symptom picture. As we look to completely match the symptom picture of the patient with the symptom picture of the remedy, it has become clinically evident that the higher potencies are more specific than are the lower potencies. Lower potencies tend to have a degree of non-specificity that allows alteration of symptoms even if the remedy is not an exact match. This can be visualized as a lock of coherency or fuzziness in the wave of the remedy. This fuzziness causes a broader area to be affected but to a less intense degree. As the remedy is further potentized, there is a sharpening of its image, an increase in its coherency, which makes the remedy more specific for the symptoms and thus more definitively acting.
Acute disease behaves a bit differently since by definition it will eventually run its course and the body can recover from its effects without dynamic intervention (unless the symptoms are dramatic enough to bring death before the disease runs its course).(8) We see this occurring because acute disease (not acute exacerbations of chronic disease) is not miasmatic. In other words it is not driven by an outside energy source. Acute disease has the energy of the initial insult or impingement, which is finite. When this dissipates, acute disease ceases to be and the body is left unimpinged. A correct remedy selection may speed this process by displacing the acute process and more rapidly dissipating it but an acute disease will dissipate on its own eventually.
Palliation and suppression can also be visualized in this model by showing points of impingement dissimilar to the points of intersection between the Vital Force and the miasm with disruptions of the patterns of interference seen between the Vital Force and the miasm. These dissimilar points change the disruption pattern on the sine wave of the Vital Force and thus alter the visible symptoms but do not compete with the miasm and thus do not remove the miasm or deprive it of its energy source.
Palliation – the sudden, temporary removal of one or more symptoms while the patient is under the influence of the medicinal manipulation and the return of the unchanged symptom when the influence of the manipulation is completed – can be seen as occurring in this model when the sine wave of the miasm/Vital Force impingement is temporarily dampened along part of its course by the medical manipulation/intervention. This will change the wave pattern to smooth some but not all of the points of impingement. When the dampening effect of the medical manipulation is removed, the sine wave complex returns to its formal state and reestablishes its former points of impingement. This allows the symptoms to be reestablished unchanged.
Suppression – the sudden and permanent removal of one or more symptoms and the subsequent deepening of disease – can be visualized as a permanent dampening influence on the sine wave of the patient, either in part or in its entirety. This would result in the removal of some points of impingement as the nature of the patient’s sine wave changed. It would also bring the apices of the patient’s sine wave and the miasm’s sine waves relatively closer together, resulting in the deepening of symptoms as we see with suppression.
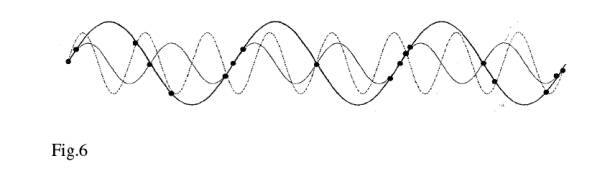
In considering multiple miasms, we can see how the symptom picture gets greatly confused. (Figure 6) As stated earlier, the primary miasm is Psora. The presence of the other two miasms depends on the presence of Psora. Thus, we can infer that Syphilis and Sycosis are contagions of the Psora/Vital Force combination. If this is true then we have secondary and perhaps tertiary sine waves superimposed. This dramatically increases the potential for the impingement of the Vital Force and increases the potential array of symptoms. As this happens, it becomes more and more difficult to match all the points of impingement with a competitive remedy. This is verified clinically in the difficulty of treating patients with multiple miasmatic involvement. Fig.6
As you can see, the use of a simple sine wave representation creates a graphic and visual model of many, if not most, of the phenomena we see in Homeopathic practice. Whether or not this model is ever used to predict the events of Homeopathy or to help someone’s understanding of the phenomena of Homeopathy is not the most critical issue. The fact that we can take a simple design from a completely unrelated field and use it as such a complete representation of the workings and predictability of Homeopathy should serve to increase the plausibility of Homeopathy to the skeptics.
References:
1. Dudgeon, R. Lectures on the Theory and Practice of Homeopathy. New Delhi:B. Jain Publishers, LTD. 1994.
2. Frankel, F. “Richard Feynman’s Diagram” American Scientist 2003; 91:450.
3. Coulter, H. Homeopathic Science and Modern Medicine. Berkley:North Atlantic Books. 1980.
4. Hahnemann, S. The Chronic Diseases (Theoretical Part). New Delhi:B. Jain Publishers, LTD. 2000
5. Kent, J. Lectures on Homeopathic Philosophy. New Delhi:B.Jain Publishers, LTD. 2002.
6. Dupree, G., Beal, S. “A Model for Homeopathy Within Allopathic Medicine and Conventional Science” Unpublished Document. 2005.
7. Dupree, G., Beal, S. “SRP: ‘Strange, Rare, and Peculiar” or “Symptoms, Remedies and Probability”?” Unpublished Document. 2005.
8. Hahnemann, S. Organon of the Medical Art. Palo Alto, CA:Birdcage Books 2001. Abstract: By following the lead of Quantum Physics we can develop diagrammatic models to help explain the workings of Homeopathy.
Key Words: Quantum Physics, Feynman Diagrams, Sine Waves
Journal of the American Institute of Homeopathy Vol. 93 No. 2 Summer 2000 pg. 89-93
——————————————–
Glen Dupree, DVM
P.O.Box 1447 St. Francisville,
LA 70775 225.721.1481