

Homoeopaths treating children have to grapple with numerous issues and problems in the field of Pediatrics. William Wordsworth encapsulated to wisdom of the ages when he said ‘Child is the father of man’. Exploring the mystery and the wonder enshrined at the core of childhood virtually corresponds to a stretch of arduous research or a random adventure for the homoeopath. How to gather case details in children when few of them are at an age to present their case articulately and coherently, is often a burning question for homoeopaths. The case-taking becomes all the more demanding in children suffering from conditions such as ADHD, retardation and autism. In order to address the complexity of case-taking in children, the other song – International Academy of Advanced Homoeopathy had organized a 2-day-seminar conducted by one of their consultant and faculty Dr. Dinesh Chauhan, on its premises on 14th and 15th June, 2014.
Dr. Dinesh Chauhan practices classical Homoeopathy in Mumbai and is well known for his pediatric cases. Insightful and passionate about Homoeopathy, he is one of the most path-breaking figures in the field of Homoeopathy today. He leads seminars in various countries and lectures on courses organized by Homoeopathic Research and Charities, the other song, WISH organization along with Dr. Rajan Sankaran and his team. The focal point of his teaching is the methodology of case-taking process which he characterizes as “the Scientifically Intuitive Case Witnessing Process”. This method is entirely scientific and easy to emulate. He heads the ABJF foundation (Non-profit organization) with his wife Dr. Urvi Chauhan where Indian homoeopaths are taught on no profit basis.
In order to provide a simple solution which could be easily adopted where case-taking in children was concerned, Dr. Dinesh Chauhan divided the seminar into parts so as to enable the audience to internalize the principles thoroughly. He started with an introduction to the general concept of case-taking, then he highlighted the methodology of case-taking in children and followed it up by important ways of how to elicit fears, dreams, delusions from non-verbal children.
He said that the best approach for most cases was Integrative Synergistic Approach which is based on the fact that what is true for one part of the system, has to be true for the whole. Supporting this, Dr. Dinesh emphasized that we can make the best of both the worlds by combining traditional, tried and true wisdom with the newest cutting-edge knowledge. The new is not only a product of the old but also a progression there from. The very founder of Homoeopathy, Dr. Hahnemann affirmed this Synergy by stating in his Lesser Writings, “How often have I wished for the concurrence of some physician of eminence on these points! I always hoped to obtain it believing that observation constructed by really practical minds must eventually unite in truth, as the radii of a circle though even so far asunder at the circumference, all converge in a common centre.”
Dr. Dinesh said that individualism, holism and similimum form the trio on which our prescription is based. But for this, every homoeopath has to understand the connection between individualization and holism. Individualized symptoms can be derived at the level of the locals, physical generals or mental generals. Holism is where all these come together be it at the level of the mind or the body. The role of the homoeopath is to find peculiar symptoms at the holistic level i.e. everything has to be individualized at a holistic level. Similarly, if individualization at holistic level is the perennial truth, then all homoeopaths (traditional, contemporary and classical) must be doing Homoeopathy at this level and they must be converging somewhere.
Dr. Dinesh then expounded Synergy in Homoeopathy conceptualized by Dr. Rajan Sankaran, where the new and the old (the system and the symptom) come together with the genius (the holistic expression running through all symptoms) to form a perfect base for any prescription. The system when used on one hand and with symptoms on the other provides a solid ground for prescription and analysis in most cases. When what we call ‘symptoms’ and ‘system’- left brain and right brain data – come together, it is like a match box and a match stick. You can add these two together – you can toss them into the same bag or drawer – and nothing happens. But when you strike them together it lights a fire. Then it is as if one plus one is not two; it is as if one plus one is a thousand. This is Synergy: when two things come together and the result is greater than the sum of its parts. Whether you first pick up the match box and bring it to the match stick, or you first pick up the match stick and bring it to the match box, it does not make a difference. When the two come together, fire is lit, the result is Synergy1.
To demonstrate the methodology which rendered the case-taking simple and practicable for other doctors, Dr. Dinesh presented many cases, some of which are outlined below. Doctor’s understanding has been highlighted in italics and the cases have been edited for brevity.
A 9-year-old boy, presenting with autistic traits first consulted Dr. Dinesh at the other song clinic. His father said that he was very restless, could not concentrate on anything, did not do any work on his own and so attended a school for special children. Everyone present at the lecture was just told to observe what was holistic in the patient and also note what was really peculiar about him. The child was given ample space and was asked what he liked to which he replied that he liked ice-cream, apple, banana, sherbet (artificial flavored drink), Pepsi, mango, sugar, Chinese food, bhelpuri. Further, the child said that he liked leg piece (chicken) (gesture). When answering, he was smiling and was very happy. It was also apparent that the child was restless.
Every child is restless. The peculiarity lies in defining the restlessness. In this child, the restlessness was mainly obvious in the legs. It is important to observe non-verbal cues as well as pay attention to verbal language. When asked to tell more about himself which was a very general open question, child started talking about likes in food, so we have to be patient and observe. The areas where gestures come up indicate energy and they have to be noted.
What was obvious was the restlessness of legs which was a part of him, and which became more apparent as the case progressed. Dr. Dinesh then took the case further trying to explore other areas, so the child was asked about his hobbies. He said that he was very fond of drawing. He likes drawing house and Ganpati (Hindu deity). The child then spontaneously said that he likes bursting crackers in Diwali (an Indian festival of lights). He also likes making a tattoo (yawning – observation).
When asked another general question, we see that the child spoke of mental state, so here we have to observe with an unprejudiced mind and try to see the connection between the physical generals expressed earlier and the mental symptoms. On observation, we see yawning at regular intervals. This too was very important in the case as it appeared frequently. Giving an example, Dr. Dinesh narrated a case of a child who was given Ferrum sulph and who imagined himself to be a warrior and wanted to learn the art of defense and save people. This child would also yawn every 2-3 minutes. It is observed that in children, this kind of behavior often denotes a defense mechanism.
Then another mental area, i.e. the fears was asked about. The child said that he was scared of horror serials and ghosts.
When children speak about dark, fear of being alone, ghosts, it is not to be considered as peculiar unless strongly present or well defined as most children will have it. The solution is to go deeper and find the uniqueness within the fears.
When asked about these ghosts, the patient replied that ghosts have black blood or red blood and he felt very afraid on seeing them. He did not stay at home and went downstairs to play when scared. When asked about other fears, he said he was afraid of monsters, who may come and hit him (gesture). He spontaneously stated that enjoyed playing in water.
Interesting to note here was that he was being asked about his fears, but from there he spontaneously veers off to areas in which he has fun. It is important to note at such junctures, where the child, despite being asked to describe something, spontaneously goes off to something else. That is perhaps the centre of such cases.
On seeing a paper in front of him, the child then enthusiastically said that he will draw a big house. On being asked to draw something that he was afraid of the child shrieked (excitedly) ‘Mummy, I am afraid of apple! Should I draw that..? I am afraid of rakshas (monster).. No, I am not afraid!’ (Excited laughter). OK, I will draw a rakshas.’
During the case-taking, it is important to remember that the child is everything; he is the director, the actor, the story teller of his other song. So, it is important that we let them take the central role. Our job is like that, of a light boy, to illuminate their other song and let it come to the foreground.
Fig 1
He drew a rakshas (Fig 1) and said that it scared him. It may hit him on the cheek. The child was then asked about his dreams. He again excitedly gestured here, saying that he did not remember them and he wanted to go home. He said that he is very scared of rakshas as he troubles him a lot (excited laughter). He again asked if he could go home.
Now this is the centre, so we have to focus on that. And not allow the patient to waver as we have to confirm.
When asked to tell more about this rakshas, the child again said that he was scared (laughing) as rakshas troubles him. The physician then asked him whether he should scare him. To this the child exclaimed loudly ‘No!’ (Restlessness of legs, laughing and peeking and making excited noises).
This is when the centre is touched and the restlessness comes up again. We have to take such symptoms and rubric which are connected to the whole. Once the centre is understood, Dr. Dinesh creates an extreme situation of fear to see the experience accompanying it. The resident was asked to show the patient a video with a car running and suddenly a ghost appeared. It was observed that the patient sat expectantly, was startled at the sight of ghost, but then immediately started laughing excitedly and came up to the resident asking to be shown another video.
If we are to see the case, we see some themes running through and through the case, one is of excitement, the other is fear and the third theme running through the case is of restlessness of lower limbs. So, we should select a remedy with excitement at the centre and having fear and restless legs as equally important components. The sphere of action should be nervous system as the child is diagnosed of ADHD. This theme of excitement is the theme of the plant family Labiatae. According to the Sensation Approach, the main sensation of the Labiatae family is excitement: vivid, pleasant, tremulous, excitement, rush of ideas, loquacity, vivacity, enjoyment, fright, anxiety, unpleasant surprises2. To match exactly the remedy from this family, each remedy from this family was scrutinized till Scutellaria laterifolia was studied and found to be matching very closely for this case.
Scutelleria – References2:
Boger – Sleeplessness from nervous excitement
Boericke – Nervous sedative, where nervous fear predominates. Nervous irritation and spasm of children.
Restless sleep must move about. Night terror.
Vermeulen
Sphere of action – nerves, A/f – emotional excitement, nightly restlessness, sudden wakefulness, frightful dreams. Fear at night in children. Nervous explosion, chilly
The child was given Scutellaria 1M. In his follow-up after a year, where he was given infrequent doses of Scutellaria, the child did much better. His restlessness was better. His attention had improved a lot, and it was apparent through his improved results in the examination. The parents were very happy with the results. He did most of his work himself and his talk was much more comprehensible. His behaviour was almost normal, so the parents and teachers were thinking of shifting him to regular school.
Dr. Dinesh then went on to demonstrate the case-taking techniques in children from age 3-16 years through approaches such that the holistic aspects of the child emerge upfront. He said that this can be achieved in most cases with an integrated, simple, scientific case-taking technique in children even with paucity of symptoms. He describes his journey along this path of establishing this technique over 8 years ago, an arduous journey which culminated in wonderful results compiled in his book, ‘A Wander with a Little Wonder’ which elaborates different case-taking approaches in children.
The basic aim of the case-taking is to elicit the PQRS (peculiar, queer, rare and strange) symptoms. Besides, the case-taking technique should also be integrative, simple, scientific, human centric and reproducible. When he was thinking how this would be possible in child cases, he stumbled across Law of Three by Gurdjieff, which stated that it is the basic for the Universe we know. And if we go deep we will find, we are bound to find that everything will be reduced to three. The whole Human consciousness, in whatsoever dimension it works, comes to ‘The Law of Three’.
Every learning, every phenomena in and around us takes 3 steps:
Step 1 – where you put lots of open ended scientific efforts but the outcome is scattered, not connected, isolated, not coordinated.
Step 2 – where things begin to co-ordinate, and get connected.
Step 3 – where all expressions get connected, coordinated effortlessly till the holistic level.
He then realized that the same thing also applied to Homoeopathy, where during the journey of case-taking, initially, we have to put open-ended, scientific, persistent efforts and in the end the whole journey becomes intuitively effortless. This happens everywhere. So, to make the approach more systematic, he divided the process of case-taking into 3 parts and named the whole process as ‘The Scientifically Intuitive Case Witnessing Process: the Journey of Three Steps.’
The first step of this journey, Step 1 is the Passive Case Witnessing Process (Open-ended scientific effort, PQRS not connected and coordinated). In this step, the child is given open, free-floating attention. The child is allowed to just be himself and express himself with ease, with minimal general interruption from the physician. You go with the natural flow and see what comes up. The emphasis is on ‘not altering the flow’. Give free floating attention.
The aim of this process is to note all the verbal and non verbal expressions that are out of place, out of order, out of content, out of proportion, out of knowledge, out of patient’s knowledge and out of any time zone. Secondly, it is also to note down all PQRS symptoms verbal as well as non verbal at physical particular, physical general and mental level. It is important to pay attention to what is common at all levels, where the two are connected, where the child is putting up defenses, or is aggravated – these become the focus. Once that is achieved, we have to start with Step 2.
The Step 2 or the Active Case Witnessing Process should be scientifically intuitive and human centric. This is the step where the peculiar symptoms from the case start coming together. E.g. in earlier case, when excitement was explored, the fear and the restlessness start coming up together. In this, the verbal and non-verbal symptoms start coming together. Here, the child may start erecting defenses as the painful part is touched. We may also notice an aggravation of physical or general state. E.g. when fears are tapped, the child may get urge for urination or may have dilation of pupils. This is the first step towards zooming into his core.
The Step 3 or the Active – Active Case witnessing Process is an Individualized or Designer’s approach to case- taking. This stage involves confirmation of the already spotted holistic symptoms through very specific questions which bring out the whole state or the experience. Once the whole is explored, in it lies everything – miasm, symptoms, source, sensation, etc. If we hold on to the thread which is common and follow it, everything gets connected.
Dr. Dinesh presented another case of a girl, of 14 years of age, athlete and a 100-metre running champion, who approached him with the complaints of recurrent damage to ligaments and hypothyroidism since childhood. She had also developed a patch of alopecia areata and had a vitiligo patch on her left temple.
Going according to the Step 1, the Passive Case witnessing Process, the child was just asked to speak about herself and the doctor waited patiently to see what peculiar things came up in the history.
The patient said, ‘I try to be the best at what I do… I try to be at the top…. I work best under pressure….I have allergy to strawberries and get cough from strawberries….(Slow talk)… I like coffee.. I like cats and dogs… and I like black colour.’ (All this was said at a slow pace, with long pauses).
‘I like listening to fast paced songs, where the beat is fast…. I used to dance but now I don’t. (Pause – thinking, eyes turned upwards.. So we have to patiently wait. After every pause something deeper comes up). I cough throughout the year… (pause)… I do not like snakes.’
We see that every pause yields something different without any repetition. We have to wait as this is Passive case receiving process.
‘I don’t like being bored at all. Bangalore is full of dead people. Unlike Mumbai which has a fast-paced life. In Bangalore, people go at their own pace…’ On waiting, some symptoms came up. After that Dr. Dinesh waited for 15 minutes more and the patient said nothing more. Till now it was an open – ended passive process. These are peculiar open ended areas, which we have to explore and see what is coming up. So we explore interests, hobbies, fears, dreams, to see what they are most attuned with.
In this case, the dreams were explored, and the patient mentioned a few dreams at a slow pace. ‘Once I was hurt and I was bleeding and at night I dreamt that the blood was green in colour and this little thing started coming out of my foot, like aliens (from a movie she had watched)..’ This was in past, but it is general, it is important why it came up in the present.
‘I was in this haunted place. There was a woman in white dress, she was stabbing herself, then a man came and pushed her. Then I got up…..’
‘I am being run down by truck and the train is coming from other side. All three of us collide. I was still alive and ran away. The truck was still following me. I went to the police station and the truck driver was arrested. I was really high, I jumped off, I thought I had a parachute when I really did not have, I was falling and I was screaming. No one heard me and after that I fell. I saw water, had to still myself. I saw a shark. I got eaten by the shark. I felt I was inside someone’s stomach and I felt I was seeing the organs. Scary. My grandfather met Hanuman. He gave some oil which I could rub on my leg and run really fast. I ran at the speed of light, very fast…’
We have to be passively alert, with all our factual knowledge. Every time we wait, something deeper bobs up.
Again the speed and light is coming up, like when and how she runs in her real life. We have to take everything together and not just what seems important. The dreams help us to understand the patient’s subconscious mind. Dr. Dinesh advised to stay with the subconscious mind longer as subconscious mind is hidden and the symptoms take time to come to the surface. In cases with paucity of symptoms, the secret is to just wait and the symptoms come up.
‘I was screeching so loudly, like an opera, that the glass broke and then the glass fell on someone and there was blood and then I saw the blood all over and then I am laughing….A big paper mountain. I was inside and someone set it on fire and then I remember a black fellow coming out. I fell, the ground was broken and I fell through…’
If we are to look at the pattern, we see injury and escape, escaping by running, high pace – running, truck, running, lack color, injury, blood and injury, someone else who is pushing, stabbing, injuring, attacking, chasing. Here we see the theme of victim-aggressor, so probably it gives a small hint of the animal kingdom. But since we are not clear, we have to repeat the question again and see where it leads.
As there were many dreams, the patient was asked one question, that is what was common in all her dreams to which she spontaneously replied that they were all about ruthless killings in which everyone and the patient dies in a different way each time, they either jumped, fell or got stabbed. Then she replied of her own accord without being asked that she was not the one killing, she was generally watching each time.
This is denial. So when asked more about how the killings occur, she says it is a different way each time, very painful. There is extreme pain, burnt, or drowning, of suffocation or blood loss. She is just standing there and watching, not going to help the victims like others. The patient reads murder stories and detective novels in which there is murder/ killing and the detective uses all tactics to solve the mystery. To see what the patient connects to, when talking of ruthless killings, she was asked what image came to her, on which she said that it is like an inhuman way of killing, like an animal. Animals are ferocious. They do not care if they are killing someone e.g. tiger killing a deer.
Here, tiger is an image, if that is the true energy then everything should come together.
‘It just attacks and tears off the flesh. Animals have instinct, they do not care as they want to eat. They do not care if they scratch or tear open any animal as they have no mercy.’ Girl is licking the table (this is known of black cats – they lick for hours at the body, so no smell of killed prey is left behind). She then wipes the area she has licked with her hands.
The Animal kingdom becomes clearer now with clear expression of victim-aggressor, you versus me theme. According to Sensation Approach, the remedies are mainly classified into 3 kingdoms – Plant, Mineral and Animal. The main experience of the plants is to do with sensitivity, of being affected and reacting. The main sensation of the Mineral kingdom is all to do with structure, whether I am lacking, if I have to complete myself, or if I am losing my structure; while the main experience of the Animal kingdom is survival.3
Power, high speed, ferocious and the black colour can be related to the energy of cats. But in order to know the source and the patient’s other song, we have to stay with the experience and confirm it.
It is important to understand that unique person sitting in front of me. ‘Let me drop everything and work on your problem’ is the motto that Dr. Dinesh adheres to when understanding a case. This becomes a part of the Active-Active Case Witnessing Process.
On being asked to describe the ruthless killing a bit more, she says ‘It is how animals kill, they just pounce on the prey (Hand gesture). It is sudden and the animal is killed. She was then asked if any animal came to her mind when she spoke of this, to which she replied the panther, though she did not know why. She said it is a black cat with weird looking eyes and she somehow felt that it was connected to her and whatever she had said. ‘Do not know much about the panther, except that it is creepy.’
This is the final bit where everything comes together. The only part left unexplored is running which she likes.
The patient was asked to talk about running and strangely, she said that she wanted to share with Dr. Dinesh about an incident, which no one except her knew. She received the last injury running in an interschool competition where she and her best friend were running together for 100 m race. She said when running, she saw that her friend was right there with her and then a micro second ahead of her. So, she speedily maneuvered her leg just a little bit so that the girl fell down and was out of action for 6 months. The coach could not make out; it was that fast she said.
We know that the cats have very fine maneuvering skills; they maneuver in the middle of fast run. All of them have power, speed, sudden attack, agility. Cheetah is known for its speed. The lion is known for his power and pride. Panther it is all in same intensity – power, speed, it is master of balancing acts. Panthers are first rate athletes (like our patient). It is the ghost of forest. Chameleon of forest. Till the end we did not realize that she will need an animal remedy. She was given the remedy Black panther.
In the follow-up after a month the patient said that she slept very well (her sleep was disturbed earlier, but she had not mentioned it). Her cough had stopped and so had the weird dreams. After 6-8 months, she said that stamina has improved. She ran 400-800 metre races easily these days, where earlier she ran only 100m. The frequency of injury to the ligaments was also much lesser. Alopecia had improved in 3-4 months, white patch also improved. She never got any dreams of attack after starting the medicine.
Dr. Dinesh then went on to explain the various case-taking methods in children who are not very expressive. A few of the case-taking approaches which can help elicit the child’s other song by using doodles, stories, dreams and drawings. He then went on to narrate a case, from the very beginning of his practice when one fellow homoeopath got his son to him. The child was suffering from status asthmaticus and many homoeopathic remedies given earlier failed to bring about the desired result.
The child was quite silent for 25 minutes and would not utter a single word. He would not share despite being coaxed and asked questions about his likes, dislikes, dreams, hobbies. The child was just watching around and suddenly said ‘Boom – Boom – Boom’ (progressively louder). Nothing else happened. Again he was pensive for sometime and would repeat the same gesture, ‘Boom-boom-boom’. Asking about this, yielded no answer from the child, so in frustration, Dr. Dinesh kept a paper before the child and then case started moving non-verbally.

Fig 2
When asked to describe the drawing, he would just gesture to keep quiet till he was done. After he completed, he ventured saying that, ‘This is the mountain, this is a man and this is a house. There is a storm and everything is getting destroyed. This has broken. Everything is being destroyed. Everyone is dying’ (Fig 2). This took 20 minutes.
As the drawing brought forth some expression from the patient, Dr. Dinesh silently placed another paper telling the child to draw whatever came to him in the moment. As the child would not communicate verbally, Dr. Dinesh found this an ideal medium to encourage his expression.
Fig 3
Then he drew another drawing (Fig 3) and said, ‘This is grass, when all go inside the grass, they do not come back. Everyone is destroyed here and only grass is left. This is a black mountain, dark. There is shrieking from here. Storm, which is bigger than the mountain also destroys everything.’
The child was asked to make yet another drawing, which he did and said that this is the biggest of all storms in which everyone dies and all buildings dissolve. Everything is destroyed. All this was said very dramatically.
Fig 4
In yet another drawing (Fig 4), he described the drawing, ‘This is a black ghost. If the storm falls in his hands, he will use the storm to destroy everything.’
We see destruction, storm, circle coming up in all the drawings. It was also observed that in all his drawings, at the centre was a blue circled thing which he filled with color. He never spoke of these circles and so this was not understood. When asked about the circle, the child said, ‘This is the cause of all destruction. Bomb. This bomb must not break. From one big bomb come the smaller ones. From one, two, from two four, from four sixteen and so on…If you don’t save these four, then all will die and only grass will remain.’
The child was then asked to describe all the drawings at once. For this, he chose to make another drawing (Fig 5) and elaborated that says that the bomb was in hands of that bhoot (ghost) and if he removes the bomb, everyone will die. In that the bomb will multiply, then no one will be able to stop it. And then he again gestured ‘Boom-boom-boom-boom’.
Fig 5
This is just similar to the chain reaction of a radioactive substance, 1 to 2, 2 to four, 4 to 16 and so on. Here we see the verbal language getting connected with the non-verbal language (what he was gesturing as boom-boom). When the radioactive substance blasts, only grass and cockroaches survive, which he mentioned later during the interview.
This gives us a fair idea that the child required a radioactive substance as the remedy. The child was sitting cross legged, which the doctor then realized that he was doing to control urination. The father came in repeatedly to ask if the child wanted to visit the bathroom. The doctor confirmed later from the father that the child sat in a cross-legged position to control the urge for urination.
On confirming the symptoms of Uranium nitrate from Phatak’s materia medica, we get Appetite – increased, Urine – holds urine by crossing his legs and then cannot control. Craving – non-veg food, Recurrent apthae in mouth. Vermeulen says that ‘Constant inclination to urinate with forcing in bladder. Had to cross her legs to prevent the urine from leaking.’4 Hence the remedy Uranium nitrate was clear and was dispensed in 1M potency.
After starting with the medicine, the child developed eruptions on the face, his asthma was a little better. The same remedy was continued and the child progressively improved each month, and the asthma finally subsided. He was more communicative now. When asked to make a drawing after a month and a year of starting the medicine, he made drawings (Fig 6) which showed the black mountain with sun shining and the trees around depicting an atmosphere of calm and peace.
Fig 6
On the second day of the seminar, Dr. Dinesh demonstrated case-taking approaches in non-verbal children, i.e. in children with autism, ADHD etc. or children below 2 years of age. Case-taking here becomes quite a challenge, due to the child’s inability to express. After persistent efforts and studying under different masters of Homoeopathy, Dr. Dinesh was able to define a methodology for such cases. He said that the portrait in such cases should always be based on the physician’s observation about the patient, where the entire focus should be on observing the natural and spontaneous behaviour of the child. The parent’s observation about the child, when carefully investigated provided useful data for forming a portrait. Mother’s history during pregnancy also plays a strategic role in such cases. The other factors which help form an effective portrait are physical examination of the child and the common pattern seen running through the history and symptoms elicited from all sources.
To demonstrate the importance of the factors stated above and their significance in non-verbal cases, Dr. Dinesh presented a case of a 18-month-old child, who was unable to speak and walk. He had developed meningitis on the 5th day after birth and was also diagnosed of having pulmonary hypertension at 4 months of age. He was in a critical state and no doctor was ready to handle his case. Thereafter, he soon developed convulsions and also had to be given oxygen for a month. The MRI shows paucity of white matter of corpus callosum.The patient slipped into coma and the doctors lost all hope, but to everyone’s surprise, he survived. He was then operated for anomalies of cardiac blood vessels and he stabilized after that. At 8 months of age, he could support his head himself.
He has episodes of breath holding where his lips became dark and bluish. One night, similarly after crying a lot, his lips turned dark and blue and then he developed a cardiac arrest. As the child entered the clinic, Dr. Dinesh observed that he turned his face towards the air conditioner and breathed deeply. This continued as long as he was in the consulting room. This we observe is air hunger. When asked about his nature, the parents said that he liked scratching and pinching people. He had a habit of throwing things around as he liked hearing the ensuing noise. When irritated, he banged his head. He is very obstinate by nature and is generally slow in all his activities.
The parents said that the child loved eating white rice and had a craving for fried things, sweets and meat, which formed their staple diet as well. Before passing stool, he had perspiration, especially on the head. The mother further observed that he did not like closed rooms and felt better in open air. After his cardiac surgery he was given oxygen for a month as his carbon dioxide levels remained high. The doctors treating him could not figure out the cause for persisting high carbon dioxide levels. This becomes all the more peculiar in homoeopathic history if it is unexplained or strange.
When asked about the history during pregnancy, the mother said that she dreamt that she was sleeping and 3 people dressed in black were strangulating her, and that she was trying to escape. Another dream was that she was in water and was struggling for breath. She felt dull and lazy all through her pregnancy and had a marked craving for sweets and rice. She felt suffocated staying with her sister-in-law and wated to get out of the house. She said that during the investigations, it was detected that the fetus had a cord loop around the neck. When the dream of strangulation was explored, she said that she felt suffocated, was struggling to come out, was breathless and she had the same experience even in the dream of drowning.
If we are to look at different aspects of the case individually, we see that the child immediately seeks the draft of air conditioner on entering the clinic. The mother also reports that he is better in open air and worse in closed room. During mother’s pregnancy history too, we see that she had peculiar dreams, where the experience was of struggling for breath. Also, after his surgery the child had to be given oxygen as his carbon dioxide levels were high which left the doctors clueless about the cause. Now we can clearly see that the physicians observation, parents observation and mother’s history during pregnancy speaks the same language, coming together. Everywhere at holistic level the experience is of suffocation, breathless, need for open air and air hunger.
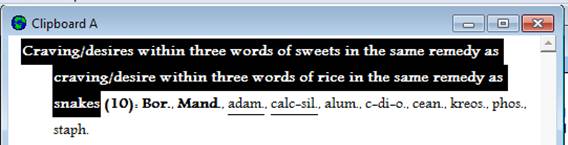
On putting some characteristic physical generals in the reference works program, Dr. Dinesh saw carbon dioxide coming up. This made him curious. We see that the child once had very high levels of carbon dioxide. Also we see laziness and dullness in mother which is central to carbons. Besides, there is a feeling of suffocation, breathlessness, as if throat is pressed and there is not enough air. So we need a remedy having carbon and oxygen and interestingly we see the desire for sweets which the mother had during pregnancy and the desire for rice both covered by Carbon dioxide. In fact, Carbon dioxide has specific desire for white rice which is exactly what our patient had. This made choice of remedy in favour of Carbon dioxide definite. He received Carbon dioxide in 200 potency.
He started walking in 8 days after starting the medicine. Not only walking but even climbing stairs. His old symptom of epilepsy came once or twice a month, so he was referred to a neurologist who did EEG which turned out to be normal. The frequency of epilepsy reduced every month, to completely disappear in 6 months time. His speech is still not clear except a few words. He received Carbon dioxide 200 once a month for first three months and then once in 15 days for next 3 months.
The main objective of the seminar was to highlight the openness and receptivity of the doctor treating a child. Since children are hamstrung by impositions of tradition, social norms, manners, they often believe reality under the pressure of inhibitions or instructions. This is where the key role of the doctor kicks in. He has to provide the patient a space and stage wherein all his fantasies, fears, dreams, visions, delusions enact their identities and their overlapping roles on the stage appropriately lit by the patient but attentive doctor.
Bibliography:
1 – Rajan Sankaran, Synergy, The Synergy in Homoeopathy – An Integrated Approach to Case-Taking and Analysis, First Edition, Homoeopathic Medical Publishers
2 – Reference Works Pro, 4.2.1.1., Michael Hourigan and David Kent Warkentin, Kent Homoeopathic Associates
3 – Rajan Sankaran, Vital Sensation and Kingdoms, The Sensation in Homoeopathy, Second Edition, 2005, Homoeopathic Medical Publishers
4 – Reference Works Pro, 4.2.1.1., Michael Hourigan and David Kent Warkentin, Kent Homoeopathic Associates
About the other song:
About ‘the other song: International Academy of Advanced Homoeopathy’:
‘the other song’ is a world class premium medical centre which puts good health and well being at the core of an academic culture dedicated to complete patient care. Situated in Mumbai, this institute is one in its kind where a team of 35 doctors headed by Dr. Rajan Sankaran (the pioneer of the Sensation Approach in Homoeopathy) come together and practice Homoeopathy. At the Academy, the students and practitioners are trained in advanced Homoeopathic practices, using new methodologies in combination with the traditional approaches, all with the use of state-of-the-art technology. The Academy is also a meeting point for different schools of thought in Homoeopathy, where renowned homoeopaths – national and international are invited, to share their knowledge and experience so that there is a constant flow of ideas on a common platform.


Pediatric casetaking some of the most difficult to take. I worked a month as a mentor to an MD in Bangkok at an Allopathic/homeopathic pediatric clinic saw only children. Some not very expressive/or verbal due to partly autistic tendency. Having them draw is a big help but you have to be able to understand their drawings,What helps is “drawings before’ remedies were given and then ‘after remedies’ during the follow up consultation.You will notice a change as the child progresses in wellness. I would also like to mention that most often with very wealthy children the mother and father do not take care of their own child,the nanny does- if you have both parents in front of you there is no response to any casetaking questions. I got a lot of replies like…. “oh you know average like all the other kids”…..(meaning the parents have no clue on what to answer due to the sad fact they have no connection to their own children) . IN these cases their caretakers often the babysitter/nanny/grandparent needs to be at the appointment.
a particular combination of symptoms is unique to each remedy. every successful homeopath has or develops his own individual method of extracting that information from patients. the variations in such methods depend on the needs of individual homeopaths considering the strength & weaknesses of individual homeopaths. Again such variations remain within certain permissible limits too. Whether these methods are useful to each & every homeopath is not guaranteed the same way a method adopted by one person to accomplish a task may not be the best method for another person who is also good at accomplishing the same task.
Apart from demonstrating the possibility of designing individual methods of case taking, I fail to understand how this method is superior to the already existing classical methods of case taking and translating the language of the patient to the uniform language of the comparison tool ie, whichever repertory or materia medica the homeopath is coversant with.
DEAR DR,
WHAT EVER METHODS, YOU HAVE APPLIED APPEARS TO ME VERY LENGTHY AND CUMBERSOME. YOU HAVE STATED THAT CHILD STARTED YAWNING. YAWNING IS A SIGN OF MONOTONY AND BOREDOM. CHILD DOES NOT WANT TO REPLY FURTHER AND BECOMES RESTLESS. A CHILD WHO CAN SPEAK SHOULD BE ASKED TWO QUESTIONS ONLY. WHAT HE LIKED MOST AND WHAT HE HATED MOST. HE MAY BE ASKED HIS 2ND OR 3RD LIKES OR HATES. I THINK THIS GIVES US SUFFICIENT CLUE TO SELECT CORRECT REMEDY.
THANKS
I agree with Dr. CSGupta. Further complicating a system is easy& everyone who knows the system can do it. What is needed is simplification & we can see the stalwarts have done only that.