


Trauma is a term that everyone has heard, and a significant number of people have experienced some type of trauma in their lives. Therefore, it is a given that many patients who seek care from a homeopath have a history of some type of trauma and perhaps multiple traumas that may be affecting them physically, mentally, emotionally, and spiritually. Trauma and violence are widespread, harmful, and costly public health concerns. Trauma affects not only the person directly exposed to it but also those around them.
It is how a person responds to the trauma that is the key to the short and long-term effects of trauma. Trauma is something that happens to a person. It is not who the person is, so it does not have to define a person’s life.
Homeopaths treat the whole person, so it is important that they understand what trauma is, how common it presents in patients, and the short- and long-term effects in all areas of a person’s life. It is part of the symptom picture for determining the appropriate remedy.
The goal of this article is to introduce the concepts of trauma and trauma-informed care to be added to the homeopath’s toolkit to enhance the practitioner’s ability to effectively treat people with trauma histories that continue to impact their lives in the present.
Definition of Trauma
Introduction
Trauma is a term that everyone has heard, and everyone has some idea about what it means. Seventy percent of adults in the United States have experienced some type of traumatic event at least once in their lives. That’s 223.4 million people (National Council for Behaviorial Health, 2022).
Therefore, it is a given that many patients who seek care from a homeopath have a history of some type of trauma and perhaps multiple traumas that may be affecting them physically, mentally, emotionally, and spiritually. Trauma and violence are widespread, harmful, and costly public health concerns. Trauma affects not only the person directly exposed to it but also those around them.
Many people think of rape, war, natural disasters, domestic violence, child abuse, etc. when they think of trauma. The reality is that trauma can be any event that overwhelms a person’s capacity to cope. They often feel fear, powerlessness, and hopelessness and may also feel that they are going to die.
It is how a person responds to the trauma that is the key to the short and long-term effects of trauma. Trauma is something that happens to a person. It is not who the person is, so it does not have to define a person’s life. The good news is that people do recover from trauma. Humans are a resilient species. We have rebounded throughout history after innumerable traumas of all kinds.
The American Psychological Association (APA) says, “Trauma is an emotional response to a terrible event like an accident, rape or natural disaster” (American Psychological Assocation, 2021). It is interesting to note that the American Psychiatric Association Diagnostic and Statistical Manual 5 (DSM) definition of trauma requires “actual or threatened death, serious injury, or sexual violence” (2013, p. 27).
That is a somewhat limiting definition given that a person’s experience of trauma is very subjective. One person may define an experience as traumatic while another with the same experience may not. The goal of this article is to introduce the concepts of trauma and trauma-informed care to be added to the homeopath’s toolkit. The article will:
- Talk about different types of trauma
- Provide an overview of adverse childhood experiences (ACEs) and their relationship to trauma and ongoing health and well-being
- Highlight the effects of trauma including changes to brain chemistry
- Discuss post-traumatic stress disorder and its symptom picture
- Provide an overview of the principles of trauma-informed care
- Discuss why this is all important to homeopaths and how they might incorporate the information into their practice
- Provide case scenarios
Let’s begin by looking at the different types of trauma.
Individual Trauma
Individual trauma is when an event happens to only one person. It can be a one-time event, or it can be multiple events prolonged over time. The Substance Abuse and Mental Health Service Administration (SAMHSA) describes individual trauma as, “resulting from an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life threatening and that has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being’” (Substance Abuse and Mental Health Administration (SAMHSA), 2019). Anyone can experience a traumatic event(s) regardless of age, gender, race, ethnicity, socioeconomic status, or sexual orientation.
Many people who have experienced trauma go on with their lives without lasting negative effects while others may have difficulties and may go on to experience traumatic stress reactions. The response to trauma is very personal. Trauma might not significantly affect the mental health of people who have strong support systems in place, little or no prior traumatic experiences, and/or many resilient qualities that can mediate the trauma experience.
According to the SAMHSA website, “Research has shown that traumatic experiences are associated with both behavioral health and chronic physical health conditions, especially those traumatic events that occur during childhood.
Substance use (e.g., smoking, excessive alcohol use, and taking drugs), mental health conditions (e.g., depression, anxiety, or PTSD), and other risky behaviors (e.g., self-injury and risky sexual encounters) have been linked with traumatic experiences.
Because these behavioral health concerns can present challenges in relationships, careers, and other aspects of life, it is important to understand the nature and impact of trauma, and to explore healing” (Substance Abuse and Mental Health Administration (SAMHSA), 2019).
Historical, Collective, and Intergenerational Trauma
“Historical, collective, and intergenerational trauma theory is a relatively new concept in public health. The premise of this theory is that populations historically subjected to long-term, mass trauma – colonialism, slavery, war, genocide – exhibit a higher prevalence of disease even several generations after the original trauma occurred” (Sotero, 2006).
“The term collective trauma refers to the psychological reactions to a traumatic event that affects an entire society; it does not merely reflect an historical fact, the recollection of a terrible event that happened to a group of people. It suggests that the tragedy is represented in the collective memory of the group, and like all forms of memory, it comprises not only a reproduction of the events, but also an ongoing reconstruction of the trauma in an attempt to make sense of it.
Collective memory of trauma is different from individual memory because collective memory persists beyond the lives of the direct survivors of the events and is remembered by group members that may be far removed from the traumatic events in time and space.
These subsequent generations of trauma survivors, that never witnessed the actual events, may remember the events differently than the direct survivors, and then the reconstruction of these past events may take different shape and form from generation to generation.
Such collective memory of a calamity suffered in the past by a group’s ancestors may give rise to a chosen trauma dynamic that weaves the connection between trauma, memory, and ontological security” (Chosen trauma: Unresolved mourning, 1997).
“Intergenerational trauma or transgenerational trauma is a collective experience that affects the group of people because of their cultural identity (e.g., ethnicity, nationality, or religious identity)” (Kolahdooz, Nader, Yi, & Sharma, 2015). Systemic racism is an example of intergenerational trauma that continues to affect people from one generation to another.
“The idea that trauma can be passed down from generation to generation is a newish one. The concept of intergenerational trauma was first recognized around 1966, as psychologists began to study children and grandchildren of people who had survived the Holocaust.
One study from 1988 found that the grandchildren of Holocaust survivors were overrepresented by about 300% (Sigal, DiNicola, & Buonvino, 1988) in referrals to psychiatric care. Researchers theorized that the effects of trauma can be transferred from one generation to the next.
This phenomenon is also known as transgenerational trauma, and when it references a shared experience among a group of people, such as Black people or refugees, it can be called historical trauma” (Zaman, 2020).
Complex Trauma
Complex trauma is exposure to varied and multiple traumatic events that are often of an invasive, interpersonal nature. Complex trauma includes sexual abuse/incest, ongoing physical or emotional abuse, chronic child neglect or abandonment, domestic violence, torture or being held captive, medical abuse or medical trauma, human trafficking, combat exposure, etc. These events are severe and pervasive, and there are wide-ranging, long-term effects of this exposure.
In her article, “Understanding Complex Trauma, Complex Reactions, and Treatment Approaches,” (2010) Dr. Christine Courtois summarizes complex traumatic events and experiences as stressors that are: (1) repetitive, prolonged, or cumulative (2) most often interpersonal, involving direct harm, exploitation, and maltreatment including neglect, abandonment, or antipathy by primary caregivers or other ostensibly responsible adults, and (3) often occur at developmentally vulnerable times in the victim’s life, especially in early childhood or adolescence, but can also occur later in life and in conditions of vulnerability associated with disability, disempowerment, dependency, age, infirmity, and others.”
According to the Center for Anxiety Disorders and Mood Disorders (2021), trauma can produce feelings of anger, persistent sadness, and despair. In addition to these symptoms, complex trauma can include:
- Change in personal self-concept
- Distrust
- Suicidal thoughts
- Episodes of feeling detached from one’s body or mental processes
- Isolation, guilt, shame, or a feeling of being totally different from other people
- Helplessness and feeling hopeless
- Becoming preoccupied with revenge or, conversely, giving total power to the perpetrator
- Self-harm, self-mutilation
- Alcoholism, substance abuse
Prolonged trauma experiences can result in extreme feelings of guilt and shame. People often feel like they are responsible for what is happening to them. It can disrupt their entire sense of self and how they interact with others and fit into the world. This contributes to isolation and hopelessness. They experience the world as unsafe, which erodes their ability to trust.
Adverse Childhood Experiences
“Adverse childhood experiences (ACEs) are potentially traumatic events that occur in childhood (0-17 years). For example:
- experiencing violence, abuse, or neglect
- witnessing violence in the home or community
- having a family member attempt or die by suicide
Also included are aspects of the child’s environment that can undermine their sense of safety, stability, and bonding, such as growing up in a household with:
- substance use problems
- mental health problems
- instability due to parental separation or household members being in jail or prison”
According to the Centers for Disease Prevention and Control (CDC), ACEs can have lasting, negative effects on health and well-being, as well as life opportunities such as education and job potential. These experiences can increase the risks of injury, sexually transmitted infections, maternal and child health problems (including teen pregnancy, pregnancy complications, and fetal death), involvement in sex trafficking, and a wide range of chronic diseases and leading causes of death such as cancer, diabetes, heart disease, and suicide.
ACEs and associated social determinants of health, such as living in under-resourced or racially segregated neighborhoods, frequently moving, and experiencing food insecurity, can cause toxic stress (extended or prolonged stress).
Toxic stress from ACEs can change brain development and affect such things as attention, decision-making, learning, and response to stress. Children growing up with toxic stress may have difficulty forming healthy and stable relationships.
They may also have unstable work histories as adults and struggle with finances, jobs, and depression throughout life. These effects can also be passed on to their own children. Some children may face further exposure to toxic stress from historical and ongoing traumas due to systemic racism or the impacts of poverty resulting from limited educational and economic opportunities” (Centers for Disease Control and Prevention, 2021).
Brain Chemistry
Most of us, on some level, know that emotional stress is a major cause of illness. The mechanism with which that happens, however, might not be something we all understand. To begin, there are three parts to the brain.
The Reptilian brain, comprised of brain stem and cerebellum, controls survival instinct (Rosenthal, 2019) and autonomic body processes such as keeping the heart beating. It is thought to be the oldest part of the brain and most likely what was most needed when early homosapiens were busy outrunning predators and focused primarily on survival.
The Neo-mammalian, or neocortex, is the newest and most evolved part of the brain; this is where cognitive processing, decision making, learning and memory take place. We use logic, make plans, create our culture and daydream from this location. The neocortex is sophisticated; it is also slower than the older parts of our brain.
In between the brain stem and neocortex lies the Mammalian brain (media co-op, n.d.), or the limbic system. This is where we process emotions. This delicate area is where fear, pleasure, and instinctive behavior are housed. When we pet a dog, it is from here that their tail begins to wag.
The limbic system contains the amygdala, which has one job only – to sense danger and set off alarms in the body when it perceives it. There is no sense of time or logic here, only response to danger. When danger is perceived, this part of the brain overrides the more complex parts, and we experience behavior that can be interpreted as fight, flight, or freeze.
When the danger alarm sounds, blood and oxygen get rerouted from the brain to the muscles; adrenaline floods the body so that we may effectively fight, flee or freeze. In that moment of danger, every system in the body not necessary for survival shuts down.
The hippocampus, part of the limbic system, is where memory is stored. When danger is sensed, this region begins to pump cortisol, rather than file our memories, which is a brilliant tactic; cortisol is what keeps us from feeling pain, so we can focus on survival.
If I get into a car accident, I might be able to walk for help before realizing my leg is broken. Once the imminent danger is over, I might no longer be able to walk on that leg. In those acute moments after the accident, cortisol release is far more important than memory retention.
The sense of danger in the body, coupled with feelings of overwhelm and helplessness can result in trauma (Leonard, 2020). Trauma can come about from the experience of a car crash, war, rape, an attack or home invasion, or any experience regardless of its size where someone is overwhelmed by something beyond their control.
Walking across a train track and hearing the bells go off indicating a train approaching could cause an acute trauma response, so long as there is the sense of imminent injury or death.
Physical, Mental, Emotional Effects
When trauma is ongoing or repeated, there can be significant effects on the physical body (Khoddam, 2021). The brain can get frozen in the sensation of being under attack.
The fight or flight reaction might remain in a near-constant state of on. Cortisol may continue to pump, even once the acute danger is over, and this heightened level of hormone increases glucose in the bloodstream. This gives an extra boost of energy should it be needed to escape danger; however, over-exposure to cortisol has harmful effects on the physical body.
The amygdala gets stuck in an activated loop, where it begins to continuously scan the world for potential threats. If the world is in fact as dangerous as the amygdala registers it, the hypervigilance could mean the difference between survival and death. However, if there is no actual threat, yet the amygdala remains on high alert, there could be negative effects on the body.
Some examples of these effects include digestive issues, headaches, muscle tension, and chronic pain. Cortisol over exposure can also be responsible for cardiovascular diseases such as high blood pressure, heart disease, and stroke. It can have negative effects on sleep, weight, memory, and concentration as well as human reproduction.
Case
A woman sought treatment several years ago for help with concentration issues and a diagnosis of gastroesophageal reflux disease (GERD). She noticed that when she was put on the nightshift at work, her stomach pains increased, and her concentration vanished.
She’d work the entire shift with what she referred to as “belly burn and baffled brain.” Several remedies were prescribed that have an affinity for such things, with very little success. As she felt more trust, she opened up about living in a car with her mother when she was young. Her mother often left her alone in the car at night while she worked. The client relayed the terror that would overtake her while she waited for her mother to return.
She then began connecting how driving to work at such a late hour brought back the same feelings of panic and dissociation she had as a child. It turned out it wasn’t the late hour per se that affected her digestion and concentration; rather, the solitary nighttime drive brought her back to a time of prolonged trauma.
Trauma can also affect mental and emotional states. Anxiety, depression, suicidal ideation, and feelings of overwhelm or isolation are common effects of chronic or repeated trauma (Substance Abuse and Mental Health Services Administration (SAMHSA), 2014). Emotional impairment, leading to unstable or unhealthy relationships, can intensify the feelings of loneliness and isolation (Ambre, n.d.).
Besides the physical symptoms of gastroesophageal reflux and weak concentration, the client also had chronic sleep issues. It generally took her hours to fall asleep and once she did, it was a fitful sleep. She usually woke unrefreshed and exhausted. Additionally, a sense of deep loneliness enveloped her, even when she was surrounded by people she enjoyed.
Once it became clear that the crux of her physical and emotional challenges was based in deep childhood trauma, I began to see the case through a new lens. My guess is that her body was stuck in a trauma loop; she would get in the car to go to work at night and be reminded of another time when she was in the car at night, alone and terrified.
Her limbic system could not differentiate the experiences. I prescribed Stramonium, a remedy with an affinity for not only gastric issues and difficult concentration, but also for deep-seated fear and chronic trauma. Over the course of almost a year, she healed her GERD, found her focus, and learned to relax into her life. Her sleep improved and her feeling of loneliness eased significantly, though it remains a work in progress.
Spiritual Effects
The spirit and the soul might also be adversely affected from repeated trauma. A loss of religious or spiritual faith seems a natural response to the belief that God or a higher power allowed such a frightful event to occur (McGee, 2017).
There might be a questioning of everything someone thought they knew of the world and their place in it after trauma. Basic trust can become splintered when cries for help are not answered. The existential sense of abandonment in those moments could lead someone to feel deserted by God/Spirit/the Universe.
This could lead to an assumption that they did not deserve the Divine love and protection they assumed would always be there for them. There is perhaps no greater sense of loss.
Post-Traumatic Stress Disorder (PTSD)
Re-experiencing
Many people with PTSD re-experience their trauma when triggered by memories that remind them of the traumatic event. Triggers could be a sound, a smell, or it could even be the way someone looks at them on a bus or in passing. Just about anything can be a trigger. When re-experiencing the trauma, individuals are thrown back into the original traumatic experience and react disproportionately.
Avoidance
The traumatic experience is so vivid that individuals overcompensate by staying away from any potential triggering situations, i.e., the sound of breaks on a bus, the sound of a siren in the street, crates falling on the ground at a grocery store, etc.
When the unpredictability of “normal” external life experiences becomes too much for one to handle, it may lead to a degree of isolation from society ranging from a mild emotional detachment from the immediate surroundings to a more severe disconnection from physical and emotional experiences. When one does not have an option and feels out of control, they may compensate with drugs, prescription or street, in order to numb the overstimulation of their anxiety.
To understand the following case, it is important to know the parameters for assessing pain. Most pain scales use numbers for 0 to 10 (Aker, 2022).
0= No pain
1=Pain is very mild, barely noticeable. Most of the time you don’t think about it.
2=Minor pain. It’s annoying. You may have sharp pain now and then.
3=Noticeable pain. It may distract you, but you can get used to it.
4=Moderate pain. If you are involved in an activity, you’re able to ignore the pain for a while, but it is still distracting.
5=Moderately strong pain. You can’t ignore it for more than a few minutes. With effort, you can still work or do some social activities.
6=Moderately stronger pain. You avoid some of your normal daily activities. You have trouble concentrating.
7=Strong pain. It keeps you from doing normal activities.
8=Very strong pain. It’s hard to do anything at all.
9=Pain that is very hard to tolerate. You can’t carry on a conversation.
10=The worst pain possible.
Case
A male veteran, 53 years of age, was referred to our clinic for chronic back pain. He arrived wearing dark glasses and avoided all eye contact with the provider. He stated that he didn’t know if he could come back to the clinic anymore after this visit because it was too difficult riding the bus with other people looking at him. He was dressed in all black with a Hell’s Angel jacket, a long thick chain connected to a wallet, and a scowl on his face.
He stated that he had been taking Oxycodone for years, but his back pain persisted, pain was an 8 out of 10 on a pain scale, with 10 being the worst. The back pain started after a car accident that happened 20 years ago. I took the symptom of the back pain and gave him Arnica.
I continued to listen to his other health issues. Ten minutes after taking the remedy, I asked him how his back pain was. He stopped, got up, moved around bending forward and backward. Finally, he said, “What did you do? I don’t have ANY pain. I’ve had this back pain for 20 years and now it is completely gone!”
As a side note, I was able to treat him in my office because homeopathic remedies are safe and do not adversely interact with allopathic medicines. He was so excited that his back pain was gone that he asked if homeopathy could help with his anxiety. He had been taking Ativan for several years for anxiety, but his anxiety continued and was increasing, with hypersensitivity to everything; noise, people, and even daylight.
After several months, he continued to come for treatment and was successfully weaned off the Ativan. He can now ride public transportation, go on long hikes during the day, and is no longer reliant on Ativan or Oxycodone.
This is just one example of how homeopathy can be used as a low-cost, successful way to treat unresolved mental, physical, or emotional trauma and how homeopathy can help people move forward in their lives.
Hyperarousal
Hyperarousal is an abnormal state where an individual is in an increased state of responsiveness to external stimuli, which brings them back to an emotional state from past experiences where they were traumatized. This leads one to a fight, flight, or freeze state of being.
Many people with post-traumatic stress live in a constant state of sympathetic nervous system hyperarousal, feeling constantly that something bad is about to happen to or near them. (Physiopedia, n.d.).
Case
A female veteran was referred to our San Francisco clinic in November 2017 for PTSD, which manifested for her in the form of anxiety, asthma, and arthritis. There were many layers to this case, and many remedy changes and adjustments as the layers came up.
With homeopathic treatment, her symptoms improved greatly. In her initial consultation, she stated that her anxiety was constantly a 10 on a scale of 1 to 10 and that she had great difficulty breathing, using her inhaler daily. With the improvement of her anxiety, her asthma also continued improving. Anxiety was steadily down to an average of 3 out of 10.
In January 2019, she came in with 0 out of 10 anxiety and depression and was sleeping well. She came in because she was going to have some dental work done and wanted homeopathic support to aid in the recovery. She continued to come in, but only about once a month or every six weeks, when something out of the ordinary would come up. Overall, she continued to go forward in life with the support of homeopathic treatment.
Fast forward to April 2, 2020, during the Covid-19 pandemic. Via a telehealth appointment, she stated, “I have anxiety, when I go outside or even think about going outside. She reported 5-7 out of 10. I feel disrespected by people coughing and not covering their mouths. It makes me so mad, which then causes a panic attack. I get anxious around people not following the rules.
I freeze with my anxiety and panic. I feel the anxiety in my whole body, from my head to my toes.” During this appointment, she did not mention any asthma attacks. We prescribed Aconitum Napellus.
In her follow-up appointment on April 16. 2020, she reported the following: “The remedy works! My anxiety is down to a 2 out of 10. I’m even doing ok when I ride the bus, which usually is very triggering. I even take the remedy inside at home if something triggers me on the news.
Life is changing, but I am adjusting with the remedy. I’m not doing great, but with the remedy, I am handling things because the remedy works immediately for me. I take it when I feel anxious or when my brain starts going crazy with all the events going on in the outside.”
Principles of Trauma-Informed Care
A program, organization, or system that is trauma-informed realizes the widespread impact of trauma and understands potential paths for recovery. It recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system and responds by fully integrating knowledge about trauma into policies, procedures, and practices. It also seeks to actively resist re-traumatization (Substance Abuse and Mental Health Services Administration (SAMHSA), 2014).
According to SAMHSA (2014), and the Trauma Informed Oregon, Regional Research Institute for Human Services, at Portland State University (2021), there are six main principles of trauma-informed care.
Safety: Safety is the hallmark of trauma-informed care. Feeling safe is fundamental to mental health and must be present for people to be willing to be vulnerable and discuss personal issues, disclose traumatic experiences, and trust that they will not be harmed.
People must feel both physically and psychologically safe. This means the physical space must be safe, and the interactions must feel safe as well. This applies to both providers and other staff. It is important to understand safety as defined by those who are being served. Privacy is also an aspect of safety. Discuss any limits to confidentiality, so there are no surprises. Part of creating a safe space includes treating everyone with dignity and respect.
Trustworthiness and Transparency: All operations and decisions are conducted with transparency and the goal of building and maintaining trust with all who receive services, their family members, and among staff, and others who interact with the organization.
People need to have clarity about expectations and how policies, procedures, and practices affect them. It is not possible to feel safe without a clear understanding of all aspects of the care they are receiving.
Peer Support and Mutual Self Help: Peer support and mutual self-help are key vehicles for establishing safety and hope, building trust, enhancing collaboration, and utilizing their stories and lived experience to promote recovery and healing.
These are key to building trust, establishing safety, and for empowerment. “Peers” refers to individuals with lived experiences of trauma or in the case of children this may be family members who have experienced trauma and are key caregivers in their recovery. “Peers” have also been referred to as “trauma survivors.”
Collaboration and Mutuality: It is important to be attuned to power dynamics and level the power differences between clients and staff and among staff as well. Healing happens in relationships and in the meaningful sharing of power and decision making.
It is important to have a true partnership between the client and the provider. Informed decision making and consent are part of collaboration and mutuality and enhance a sense of safety. Everyone in the organization has a role to play in a trauma-informed approach.
Empowerment, Voice, and Choice: Everyone who encounters the clients builds on what clients have to offer rather than responding to their perceived deficits. Their resilience, strengths, and experiences are recognized and built upon. The focus is on “what happened to you” versus “what is wrong with you.
People who work with people with trauma histories need to be able to tolerate strong reactions to include fear and anger, uncertainty, and not being able to fix it. Everyone in the organization needs to be aware of their own biases and responses.
Services should be flexible, individualized, culturally competent, gender responsive, and promote respect and dignity. They should be based on best practices and reflect the centrality of trauma in the lives of people who receive services, people who provide services, and staff who support them.
People need to have a voice and choice in determining what happens to them. Otherwise, they are likely to be re-traumatized. That is the opposite of empowering a person to take back control of their decisions and lives.
Cultural, Historical, and Gender Issues: It is important to understand clients and their experiences in context (across the lifespan, cultures, and societies). Organizations providing trauma-informed care must move past stereotypes and biases (e.g., based on race, ethnicity, sexual orientation, age, religion, ability, gender-identity, geography, etc.), offer cultural and gender responsive services, leverage the healing value of traditional cultural connections, and recognize and address collective and historical trauma such as systemic racism and genocide.
Providers should be sensitive to leveraging the healing value of traditional cultural connections and healing modalities. Everyone in the organization needs to be aware of their own biases and stereotypes and be doing their individual work to effectively engage in the work to dismantle systemic racism that exists in every institution.
Treating Trauma with Homeopathy
In the United States, there are a very significant number of people who have limitations due to personal trauma, or cultural and/or intergenerational trauma. Anyone of us including practitioners can be struggling with the profound effects of trauma on our lives and health. Homeopaths can assume that any of our clients may have had traumatic experiences during their lives.
Our clients may have unconsciously suppressed traumatic events, so they may be unaware of their trauma. In more extreme cases of subconscious trauma, they may not even be aware if they are currently or intermittently experiencing PTSD.
Even when clients are aware that they have a history of trauma with resulting lasting limitations, we homeopaths as partners in healing, want to avoid triggering any client during the very personal homeopathic interview. One of the foremost principles when helping to heal trauma, is creating a safe, trustworthy therapeutic relationship wherein we are not causing further harm to a person inadvertently.
From a homeo-therapeutic perspective, it is not necessary to know the details of a person’s trauma to find a helpful or even a curative remedy. We should never press or even suggest any client talk about the details of a traumatic event or state. If someone tells us their story of trauma without our asking them, we must be able to hold space for that, as talking about it may be what is needed.
Homeopaths should be conscious of the inherent power dynamic between any practitioner and patient/client. Specifically for clients with trauma histories, we should realize that there is likely to be a tendency for people to state the facts of what happened automatically, if they assume that we need to know that information.
Therefore, it is up to us to be clear about what information we need to help them homeopathically. We can do this generally at the start of the session and especially if we sense trauma is coming up during the session. We can share that it is much more relevant how they have coped and adapted despite the trauma.
Also, of course, important is the nature of their ability to be free and present physically, mentally, and emotionally. If those freedoms are currently compromised, we observe the nature of those limitations. We need to ask about those limitations in the most respectful and collaborative way, and over a time frame that feels appropriate to our client, if indeed they decide to share about that directly.
It’s also important for us to have some awareness of the situation of the people we are treating, especially if we are working with a specific vulnerable population. For example, un-housed people are exposed to ongoing violence, dehumanization, and other traumas in the environment, which can trigger past trauma in an ongoing way.
Another example is a person who has recently or in the past experienced a natural disaster or other acute trauma. Unfortunately, these seem to be becoming more common. I have volunteered my homeopathy services with the Integrative Healers Action Network for people impacted by wildfires in Northern California since 2018.
I have learned a lot about how to help people homeopathically who may be currently in acute trauma but who are likely to also be having past traumas triggered in the moment and who may continue to be limited in future by cumulative, complex trauma – especially for people with very little resources and/or other health issues.
The following graph (FEMA and U.S. Department of Health & Human Services, 2021) helps to illustrate some of the typical, natural human responses to a traumatic event.

The next graphic (Berry, Clarke, Fleury, & Parker, 2014) demonstrates the complex nature of the experience of people impacted by climate change-related disasters such as the wildfires.
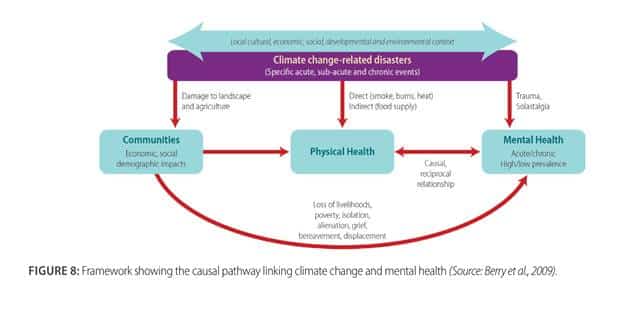
When we consider the likelihood of certain populations to have experienced many traumatic events in their lifetime, we can imagine that (simplistically) there may be many such timelines of emotional highs and lows overlaid, not only one.
As such, there is much more nuance and compassion required for understanding the “common” response timeline to trauma so that we can more easily discern what is more specific to the person, which is how we can help find a good remedy. We homeopaths know that the compensation for trauma can be expressed in a very wide range of ways: physical, emotional, mental, and spiritual.
Multigenerational or ancestral trauma is that which was experienced by ancestors and passed down and expressed epigenetically in an individual. That person may have a wide range of expressions of this trauma, from memories which are not theirs, to strong anxiety and depression from a young age with feelings of danger, despair, or depersonalization that are out of proportion to their lived experience.
Another possibility, much like people who have a high number of ACEs, there can be serious disease developed early in life. We recognize that as the syphilitic miasm in homeopathy, broadly speaking, but it can also indicate ancestral trauma.
To serve people who have or are likely to have a history of trauma responsibly, we want to always be thinking about the basic principles of trauma-informed care and applying them proactively, being homeopathic to the individual. Some specific things to consider:
- If you, yourself, have a history of trauma that you are aware of and have not addressed it adequately, please work with a qualified therapist and/or homeopath or other holistic or somatic therapist and be aware of your limitations.
- Even if you do not have a history of trauma, if you regularly work with clients with serious trauma, you will likely need to be very proactive with your self-care. Trauma is a lot to hold space for, and it can easily take a toll on us as practitioners.
- Create, communicate, and hold good boundaries. This is important with all clients of course, but especially important with clients with trauma who can be very sensitive, or even have cognitive and logistical issues that mean they may take longer than others to learn/understand your practice boundaries.
- Hold the consultation in a safe (to them) environment. For many people, this will be in a private office setting. However, if this is a person who doesn’t feel safe being indoors, has sensitivities that preclude them from travelling to your office, or has experienced medical trauma and may not be comfortable in this setting, accommodate them with other options if you can.
- Be familiar with trauma-informed psychological first aid and be ready to provide stabilization techniques, such as training with HeartMath Institute, and The Red Cross.
- While we are always matching the remedy to the whole person and largest totality of symptoms, respect that for a client with trauma, much of that current symptom picture may be observable, and we can think of the goal as helping them to become better resourced in the moment, asking them what help they need the most.
- Be aware that if you are expecting the person to take a homeopathic medicine with regularity outside of the time you are with them, have clear, written communication about this in a format they can access: written and/or on a device and/or on the medicine container. Make sure the medicine is in a form that they can keep track of and self-administer.
- Communicate which medicine, including potency, you are recommending, why you are recommending it for them, and where it is available that is accessible to them in the future. This is a key feature of safety and non-dependency, which signals trust in the restoration of resilience of the individual.
While we may want to emphasize that people may not need this same medicine again in the future, especially on an ongoing basis, it’s important to establish that the medicines are available and that we are not the only source, and what may indicate a need for this remedy again in the future.
Better still is if we can help them understand additional accessible ways to work with a homeopath, especially if we have limited availability for the person. This is more likely to be the case in acute trauma clinics, such as with the Integrative Healers Action Network.
Homeopathy for Trauma Case Examples
All names have been changed to protect the identity of the clients, who have all given their permission to use their case as an example.
Case 1: Trauma Affects Mental Ability and Experience of Pain
Deborah is a 65-year-old woman artist who came to my neighborhood homeopathy clinic for seniors in 2015. She is a thin Israeli woman with lots of moles and freckles. She has lived in the U.S. for most of her adult life. She has long relied on over-the-counter homeopathic remedies, as she is very sensitive to conventional medications of any kind, having had allergies to several kinds of commonly prescribed drugs.
Her main problem she wanted help with at that time was a several year-old foot injury caused by a city bus handicap ramp landing on it. She also mentioned her ongoing irritable bowel syndrome (IBS), debilitating arthritis with nodules especially in her hands which she needs for painting her art, poor memory “word dyslexia” when in pain, bone spurs on the foot, and fibromyalgia.
It took maybe six months of follow up before she shared with me about her significant trauma history; however, she demonstrated many hallmarks of the impact of trauma during the intake.
She seemed very discombobulated to me when she first came in, so much so that I wondered about her mental health. She talked very fast, describing health issues or memories that I wasn’t sure when they were from. I found myself having to breathe deeper and slower just to keep calm, as she seemed very upset and ungrounded.
I took her case before I began working with the Integrative Healers Action Network, where I have learned that this might have been a good time to do some grounding work with her for a few minutes, coaching her through some simple breathing exercises with me, or increasing somatic awareness of her feet on the ground, sitting in the chair, or breathing in an out in the current moment together.
Likely, that would have helped her to communicate with me more clearly about her current issues. On the other hand, I believe this was her chronic state for quite some time and so that approach may have been of limited value and may have seemed strange to her having just met me.
She told me she had gone to a grief therapist and was in shock after her husband died three years ago, right before her foot was injured by the bus. “I wasn’t in my right mind. Then my cat died (very big grief), then my phone landed on the same spot (on injured foot).” “Every single part of me hurts every day. Emotionally I feel terrible. Ongoing injury. Bone spur is like something pushing at me like the fibroid I have on the left side; it’s shrunk now. I’m crooked from my injuries and fibroid.”
She has had arthritis since her 30s, and fibromyalgia… “the doctor didn’t believe me.” This is a big theme, doctors not believing her pain level or sensitivity to meds, which unfortunately is still a very common experience for women from their medical providers.
Her arthritis is much worse in cold weather, and she is generally worse from cold and damp and much better in the sun. Generally, she is cold all the time, then suddenly hot.
She can have burning or even stabbing joint pains, worse at night, when she has a lot of inflammation, such as when her allergies are affecting her. She still gets period symptoms though she’s been through menopause for years.
Her IBS started when she wanted to divorce her abusive ex-husband. She can get blood in her stool with it and bloating. “I was also working in social services. I don’t have the temperament for that, my nerves are too high – I have fire energy that I use in my art. I can get burned up in it.”
She’s also had issues with bleeding gums.
She grew up in Jerusalem when the city was divided. She can freeze up from sensed tensions in situations because of this tense place in her upbringing.
I notice there is a lot of energy and expressive motion in her upper body, with her hands and arms, moving up and out as she’s telling me her history. She has a lot of energy even though I can tell she is in a lot of pain. She never stops talking during the interview time.
“When I’m painting, I get so involved I can forget the pain. I can be on; it brings out the best in me. For myself, I can’t turn that on.”
She gets some allergies year-round, watery eyes and headache, pressure coming in at the back of the head and over the eyes, worse from any pressure. She has a chronic cough with allergies and sometimes wheezing. She can have lingering coughs after a sickness, worse at night and worse lying down.
She talks about being very bothered by any pressure of restrictive clothes like her bra. This is worse during “her cycle” when her breasts get swollen.
I thought Phosphorus might be a good remedy to begin to help her to be more integrated with her experiences, including her profound history of grief, which was clearly still affecting her. The Tubercular miasm seemed quite strong, with a restlessness that was evident. Phosphorus seemed to also fit her strong sensitivity, hormonal influence, and tendency to bleeding gums and colon with inflammation and stress, though definitely there are strong snake remedy indicators as well.
I recommended Arnica 10M pellets and Phosphorus 30C in water daily each, at opposite ends of the day. She was told to reduce in frequency if she has dramatic improvement.
Two weeks later, we had a brief consult at clinic. I am taken aback by how different she seemed! She was much more coherent. We had a conversation this time.
“Arnica has really made a difference! Took it every day and then every other day, and now just as needed if I will be on my feet a lot that day. Phosphorus worked really well the first few days, less wheezing less achy-ness in foot. Allergies have been more intense with the good weather and pollen! But at least I’m not wheezing.”
I added weekly Tuberculinum 200C to her regimen.
At the one month follow up in clinic, again she was much more coherent, like a different person from the intake appointment.
“I’m healing. I can touch my foot, massage it. It’s a lot better. Tuberculinum, I felt a major difference the day I took it, for my allergy symptoms. I am only taking the Arnica if I have a day where I must do a lot of standing or walking, otherwise not in much pain. The Arnica has really calmed the inflammation down.”
Her foot healed fully within another month, after having been chronically painful and enflamed for three years. As we have worked together, she has had many different remedies which have helped a bit with her chronic joint pains and allergies, including almost all of the nosodes, a few different snake remedies, Lac Maternum and Lac Felinum, Phosphoric Acid and Ignatia after new grief.
She still takes Arnica occasionally, and Rhododendron helps reliably when her arthritis flares up with cold weather. Calcerea fluorica 6C we’ve newly discovered helps her hands specifically not to be as stiff.
I learned more about her over time, that she is extremely impressionable and tuned in to what others think and say. Despite that sensitivity, she really needs to be able to be around people, to connect (and to talk!). The pandemic drastically affected her mental health for the worse, not being able to be around others very much or show her art.
She gets anxiety-induced asthma from wearing a mask, and there has been a local mask mandate for over a year and a half, including outdoors for most of the time. Her anxiety went off the charts during this time, and I observed a return of the lack of coherence in our conversations for the first time since her intake. Higher potencies of the remedies that had helped her in the past did not help, but long conversations did seem to help her temporarily.
In late 2020 and into 2021 after hearing of many friends and some family passing away or having serious strokes in Israel, she believes soon after taking the COVID-19 vaccines, she was very anxious and depressed. She said her family tried reporting some of the injuries and were told that the person was just old, and it wasn’t related to the vaccine. This triggered her longstanding medical trauma of iatrogenic illness due to her sensitivity and not being believed.
She also shared with me more of her history of trauma growing up, which I will not detail, but there was abuse when she was young that was covered up. She also felt responsible as a child for pointing out to her brother where bombs were still in the countryside and hoped that he would heed her warning and come back from playing unharmed. This history still lived in her nervous system she admitted, with resultant hypervigilance and a pessimistic fear of authority figures taking advantage of her.
I thought about the gemstone remedies, because of their potential to help people who have been carrying trauma for a long time, with the theme of being grounded or ungrounded (she alternates very dramatically depending on her pain level), and the theme of abuse, betrayal, violence, and protection.
Looking closer at the gems, Amethyst Immersion stood out to me as a good candidate, as it can be indicated for those who are very sensitive, including to what others think of them and generally picking up on others energy too much. It has an affinity for the nerves, lungs and sinuses (Tumminello, 2011).
I recommended Amethyst Immersion 1M in liquid form so that she could succuss (increase the potency slightly by shaking the bottle) the remedy and repeat it if needed with less chance of aggravation. Surprisingly, for being very sensitive, she seems to tolerate remedies in C scale well, even taking them often, such as multiple times a week.
Two weeks later she is the most grounded I have witnessed, maybe ever since working together, and I’m quite surprised, as she is still having a lot of stress. She tells me that the Amethyst has made a tremendous difference for her anxiety, and mentally she feels much better.
She’s not worrying about things that she can’t control, and she’s able to do her art, and go for walks on the beach and appreciate life again. She realized that the mask made her feel like she was trapped under the table when she was a child, hiding from her parents when they fought. She found another solution, a face shield, and got a medical exemption for it so that she could go shopping if need be (a friend had been shopping for her, but it was stressful to be that dependent).
Her allergies got much worse, even as everything else seemed to improve greatly. However, now it was more sinus symptoms, not wheezing. I waited some time to see if this could improve, as it seemed this is in the direction of cure. Eventually, she did well with Kali Iodatum 30C for her allergy symptoms.
I recommended that she repeat the Amethyst Immersion 1M (in tincture) quite a few times when she feels her stress and anxiety returning, and it worked very well. Her allergies were not as bad. She got much healthier mentally and emotionally, and I would say that she gained a lot of perspective about past events.
Most recently in 2022 and early 2023, she has gotten profoundly better from the remedy Crotalus Horridus, which I finally thought of for her based on her mental limitations during times of trauma re-triggering, her forsaken feeling (which is a snake theme), bleeding gums and bloody stools at times, and memory issues which are significant.
She has progressed to a 10M of Crotalus Horridus, and for the first time in our many years of working together, she has become more independent of me and others, secure, much less anxious, and all of her physical ailments are less bothersome. I believe this may be a constitutional for her for quite some time.
Case 2: Breaking the Cycle of Family Trauma for Healthier Parents and Parenting
Anne was in her mid-30s when we began working together in 2018. She had had a medically complicated traumatic birth two years prior, though was happily parenting her two-year-old, together with her partner. Their child, Sam, had suffered brain injury during birth and had some neurological and developmental challenges, for which they have found very good therapists, and made great strides. Additionally, Anne had a family history of alcoholism and mental illness, which had left some deep patterns of trauma response around parenting for her that can get triggered.
When she first came to see me, she wanted help with her anxiety, which felt directly related to sleep deprivation from the early years of parenting. “I still have days where I feel pretty anxious, like I’m not in my body, like I’m going to pass out or lose my mind. In the past I’ve felt panicked while driving or flying or in a crowded space or a long line (feeling trapped). I haven’t had heart palpitations in about a month.”
“We want to try for a second. The doctor said you’re going to want to be monitored… upset by all the things she said. I’ve been too afraid to get questions answered from my midwife.”
“Tighter and more tense in my body, don’t take full deep breaths. Hyperventilation almost.
A month ago had an early miscarriage, heart palpitations since then.”
“Feel tired, tense. Fears around… I can’t handle this. I’m going to pass out, going to have a psychotic break.”
“Stacking on old experiences with my mom, done Eye Movement Desensitization and Reprocessing (EMDR) to help with that. Dissociated, not in my body. I need to be sitting in a quiet space. I avoid driving in heavy traffic or long lines or flying or even waiting in line.”
“Ancestral fear…afraid I’m not going to be there for Sam. Like my mom wasn’t there.
“Family stress, hospitalizations for my mom… she thought we had poisoned her. I get a lot of disturbing images from different stressful experiences in past. Is it safe for me to feel all of this? Needing to feel grounded in my body and allow normal, healthy emotions to come through. Get a crawling feeling in my legs before panic attack.”
Anne has a history of upper respiratory infections, once had walking pneumonia, but is much better since no longer being vegan. Her menstrual cycle was regular, and she had noticeably more anxiety before it, and sadness with weepiness during. She also had looser stools in the first part of her cycle.
Sepia 30C helped her to feel quite a bit better, repeating a few times per week, if she felt anxiety, in the first month. At that time, increased to 200C, as her anxiety can still spike quite high and she’s very afraid to drive still.
At the two-month follow up, after holidays with typical eating rich and sugary foods, drinking wine, and coffee, she is not seeming very well. She’s still nursing and not getting enough sleep. Her digestion is off, not surprisingly, but it seems the anxiety is still quite high though she is not having heart palpitations.
“Afraid of that feeling of losing control. Old trauma with my mom’s hospitalizations, not knowing when she would come out of a facility. So protective of Sam. Are these feelings too strong? What if I’m not getting help that I need (like her mom didn’t)? It’s my ultimate fear.”
I feel floaty, not in my body… rung out. It’s hard to relax.”
Lac Maternum 10M shifted things in an important way… “felt a little easier to reframe during anxiety, a little more space emotionally around things that have been feeling hard. Feeling a little more patience and presence with Sam, more able to see my way through a struggle. More energy for things.”
Things were better for some time and then worse again, and we had a follow up many months later.
“A week ago I was ready to have them commit me…images of knives, really scary. I tracked down old doctor who said intrusive thoughts could be memories. Realized my mom had been having a break when I was in my early 20s. This could be healing old trauma. Feeling alone and isolated, night weaning. Fear to be alone with Sam. When I’m alone at night, thought of a knife, what if brought it upstairs… Vacillate between fear of something happening to Sam when he’s with the babysitter and hypervigilance.”
Sepia 1M, breathing exercises, and EMDR all helped very much within a week. She was able to have space from intrusive thoughts and from her anxiety.
She was well supported by Sepia 1M taking it 1-3X per week for over six months, and then Sepia 10M to support her as she took a new more challenging job. She still had occasional intrusive thoughts but was very healthy and wanting to have another child.
Sepia 10M and occasional Carcinosin, and a few other acute remedies made a very big difference, supporting her through a miscarriage, and like so many others, anxiety and fear during the pandemic.
Then last December, with cumulative stressors from work and stress of wanting to get pregnant but not totally sure she can handle it, the intrusive thoughts flared up again. Her panic and anxiety have remained much improved, but this is not in the direction of health. Intrusive, especially violent thoughts are a deeper disturbance of the vital force than anxiety or panic attacks, even though they do not occur often.
“When alone with Sam, flashes of – I’m in charge of him…what if I snap and hurt him? When doing the listening, patient parenting… Mind flashes into this is why people beat their kids. Less worry that I’m going to, but graphic images of the terrible things other people do… oh, I bet people would poison kids. Maybe wonder about past life thing. Why am I thinking about it…”?
“What if something happens to me, and Sam and I are alone? What if have a heart attack and then Sam is traumatized by that?”
I considered higher potency of Sepia, Pulsatilla, gem remedies… but decided on Thea sinensis, as this remedy specifically has such very strong impulses, in addition to graphic violent images of children, in the homeopathic proving. It also had a strange physical symptom she had recently developed, roaring in the ear sound upon rising.
Thea sinensis 1M greatly reduced her intrusive thoughts.
She’s made it through the recent death of her father with great spiritual perspective, and a couple of doses of Ignatia 10M were supportive during that week.
Anne is over 20 weeks pregnant, and navigating challenges of work life balance, but overall doing very well on all levels. She is currently taking Thea sinensis 10M (tincture, plussed) occasionally. Occasionally, she has a fearful intrusive thought, but she has a lot of emotional space from it and is able to let it go quickly.
Working more with trauma, both acute and chronic, has taught me to more easily recognize it in individuals and in the collective. I observe that the ongoing pandemic has induced collective trauma in our nation, and I suspect, globally.
Locally and globally, devastation due to more extreme climate events (wildfires, floods, tornadoes, heat waves, etc.) has produced individual and collective grief and trauma. And that is without the political polarization that is gripping much of society, adding to people’s anxiety and stress.
I have compassion for humanity in the moment we are in and am so grateful to be able to help people with homeopathy during this challenging time of great change. I hope that sharing some of this experience encourages more homeopaths to learn about trauma, so that we may all continue to help our clients who are trauma survivors to be more resourced, and to heal. I am continuously impressed with beautiful human resilience, the vital force in action. When people are reminded of their ability to heal at this profoundly deep level, it is extremely empowering.
Authors
Sandi Kaplan, CCH, PCH
Kathleen Scheible, CCH
Wanda Smith-Schick, CCH
Glenna Tinney, MSW, ACSW, DCSW
References
Aker, J. A. (2022, August). Your Pain on a Scale of 1-10? Check Out a New DOD Way to Evaluate Pain: Defense and Veterans Pain Rating Scale. Retrieved from Military Health System and Defense Health Agency: https://www.health.mil/News/Articles/2022/10/13/DVPRS-pain-scale
Ambre, D. K. (n.d.). The link between childhood trauma and adult loneliness. Retrieved from Ambre Associates: https://www.ambreassociates.com/blog/childhood-trauma-adult-loneliness
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Arlington, VA, USA: American Psychiatric Association. doi:https://doi.org/10.1176/appi.books.9780890425596
American Psychological Assocation. (2021). Trauma. Retrieved from American Pychological Association: https://www.apa.org/topics/trauma
Berry, P., Clarke, K.-L., Fleury, M. D., & Parker, S. (2014). Chaper 7: Human Health. In F. J. Warren, & D. S. Lemmen (Eds.), Canada in a Chaning Climate: Sector Perspectives on Impacts and Adaptation (p. 286). Ottawa, ON, Canada: Government of Canada. Retrieved from https://www.nrcan.gc.ca/sites/www.nrcan.gc.ca/files/earthsciences/pdf/assess/2014/pdf/Full-Report_Eng.pdf
Centers for Disease Control and Prevention. (2021, Apr 6). Violence Prevention: Preventing Adverse Childhood Experiences. Retrieved from Centers for Disease Control and Prevention: https://www.cdc.gov/violenceprevention/aces/fastfact.html
Chosen trauma: Unresolved mourning. (1997). In V. D. Volkan (Ed.), Bloodlines: From Ethnic Pride to Ethnic Terrorism (pp. 36-49). New York, NY, USA: Farrar, Straus, & Giroux.
Courtois, C. A. (2010, Jun 10). Understanding complex trauma, complex reastions, and treatment approaches. Retrieved from Gift From Within – PTSD Resources for Survivors and Caregivers: https://www.giftfromwithin.org/html/cptsd-understanding-treatment.html
FEMA and U.S. Department of Health & Human Services. (2021, Jun). FEMA Crisis Counseling Assistance and Training Program Guidance, CCP Application Toolkit, Version 5.2. Substance Abuse and Mental Health Services Administration (SAMHSA). Retrieved from https://www.samhsa.gov/sites/default/files/dtac/ccptoolkit/fema-ccp-guidance.pdf
Fowler, D., Hodgekins, J., Garely, P., Freeman, D., Kulpers, E., Dunn, G., . . . Bebbington, P. E. (2012, Sep). Negtive cognition, depressed mood, and paranoia: A longitudinal pathway analysis using structural equation modeling. Schizophrenia Bulletin, 38(5), 1063-1073. doi:10.1093/schbul/sbr019
Khoddam, R. (2021, Mar 3). Trauma: How trauma affects the body: Learn how trauma affects the body and treatments to help you. Retrieved from Psychology Today: https://www.psychologytoday.com/us/blog/the-addiction-connection/202103/how-trauma-affects-the-body
Kolahdooz, F., Nader, F., Yi, K. J., & Sharma, S. (2015, Jul 16). Understanding the social determinants of health among indigenous Canadians: Priorities for health promotion policies and actions. Global Health Action(8). doi:10:3402/gha.v8.27968
Leonard, J. (2020, Jun 3). What is trauma? What to know. Retrieved from Medical News Today: https://www.medicalnewstoday.com/articles/trauma
McGee, V. (2017, Dec 6). The Blog: Trauma and restoring faith. Retrieved from Huffpost: https://www.huffpost.com/entry/trauma-restoring-faith_b_8959580
media co-op. (n.d.). NHS Lanarkshire’s EVA Services: Trauma and the brain. Retrieved November 2021, from media co-op: https://mediaco-op.net/projects/nhs-lanarkshires-eva-serviceanimation/
National Council for Behaviorial Health. (2022). How to manage trauma. Retrieved from National Council for Mental Wellbeing: https://www.thenationalcouncil.org/wp-content/uploads/2013/05/Trauma-infographic.pdf?daf=375ateTbd56
Physiopedia. (n.d.). Vagus nerve. Retrieved from Physiopedia: https://www.physio-pedia.com/Vagus_Nerve
Rosenthal, M. (2019, Jun 27). The science behind PTSD symptoms: How trauma changes the brain. Retrieved from Boston Clinical Trials (BCT): https://www.bostontrials.com/how-trauma-changes-the-brain/
Sigal, J. J., DiNicola, V. F., & Buonvino, M. (1988). Grandchildren of survivors: Can negative effects of prolonged exposure to excessive stress be observed two generations later? The Canandian Journal of Psychiatry, 33(3), 207-212. doi:10.1177/070674378803300309
Sotero, M. M. (2006, Fall). A conceptual model of historical trauma: Implications for public health practice and research. Journal of Health Disparities Research and Practice, 1(1), pp. 93-108. Retrieved from https://www.researchgate.net/publication/228209032_A_Conceptual_Model_of_Historical_Trauma_Implications_for_Public_Health_Practice_and_Research
Substance Abuse and Mental Health Administration (SAMHSA). (2019, Aug 2). Trauma and violence. Retrieved from SAMHSA: https://www.samhsa.gov/trauma-violence
Substance Abuse and Mental Health Services Administration (SAMHSA). (2014). Chapter 3: Understanding the impact of trauma. In A Treatment Improvement Protocol (TIP) Series, No. 57: Trauma-informed care in behavioral health services. HHS Publication No. (SMA) 13-4801. Rockville, MD, USA: Substance Abuse and Mental Health Services Administration. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK207191/ or https://www.ncbi.nlm.nih.gov/books/NBK207201/pdf/Bookshelf_NBK207201.pdf
Substance Abuse and Mental Health Services Administration (SAMHSA). (2014). SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach, HHS Publication No. (SMA) 14-4884. Rockville: SAMHSA. Retrieved from https://ncsacw.samhsa.gov/userfiles/files/SAMHSA_Trauma.pdf
The Center for Treatment of Anxiety and Mood Disorders. (2021, Sep 15). Complex Trauma Disorder. Retrieved from The Center for Treatment of Anxiety and Mood Disorders: https://centerforanxietydisorders.com/complex-trauma-disorder/
Trauma Informed Oregon, Regional Research Institute for Human Services, Portland State University. (2021). Trauma informed care principles. Retrieved from Trauma Informed Oregon: https://traumainformedoregon.org/resources/new-to-trauma-informed-care/trauma-informed-care-principles/
Tumminello, P. (2011, Feb). Introduction to the gem family. Retrieved from Interhomeopathy: http://www.interhomeopathy.org/introduction-to-the-gem-family
Zaman, M. (2020, Jun 1). What is intergenerational trauma? An expert explains. Retrieved from Refinery29: https://www.refinery29.com/en-us/2020/06/9848448/what-is-intergenerational-trauma


