

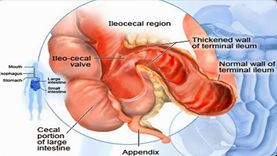
CROHN’S DISEASE
Crohn’s disease is a non-specific infection of the terminal ileum, hence the name regional ileitis.
AETIOLOGY
- Reticulosis- the hypertrophy of the reticular tissues of the bowel during the acute stage has led to the inception of this theory.
- Infection- (a) Streptococcus, coliform bacteria or virus.
(b) Ingestion of toothpaste may play some part in chronic irritation.
PATHOLOGY;
- Crohn’s disease is progressive granulomatous lymphangitis, which produces cicatrization and ulceration of the mucosa.
- In the chronic stage, hyperaemia is minimal but the intestinal wall feels quite firm (like hose pipe).
- Mesenteric lymph nodes are enlarged, and the mesentery is also thickened and enlarged.
MACROSCOPIC
- Mucosa shows multiple ulcers and inflammatory oedema.
- Submucosa thickened due to lymphedema and subsequent fibrosis.
- Often there may be perforation leading to diffuse peritonitis or there may be an external or internal fistula.

- Mesentery- thickening and oedematous in the acute stage.
- Mesenteric lymph nodes are enlarged.
- In this stage, there is stricture or formation of a lump.
- It appears like hyperplastic ileo-caecal tuberculosis.
CLINICAL FEATURES:
- STAGE 1
- Common in young adults with a peak onset between 20 and 40 years
- Diarrhoea with or without colicky pain
- Pyrexia
- Tender mass in the R.I.F
- Slight anaemia
- Blood and mucus in the stool
- Peri-anal inflammations.

- STAGE 2
- Obstructive signs(signs of chronic or acute on chronic intestinal obstruction)
- Malabsorption due to extensive involvement of the bowel with Steatorrhoea and multiple vitamin deficiencies.
- STAGE 3
- Slow perforation of the intestine with the formation of fistulae in the adjacent loop, bladder, or skin.

RADIOLOGICAL CHANGES;
- The outline of the ilium may be indistinct with oedema of the wall.
- Straightening of the valvulae conniventes.
- Cobblestone reticulation (when there is ulceration)
- Constricted terminal ileum (string sign of Kantor).
TREATMENT;
CONSERVATIVE – As per the surgical approach this is for the improvement of general health and is never curative, but as a homoeopath, I would claim that we have quite a good scope in treating the said condition and would succeed in curtailing the progress of the disease.
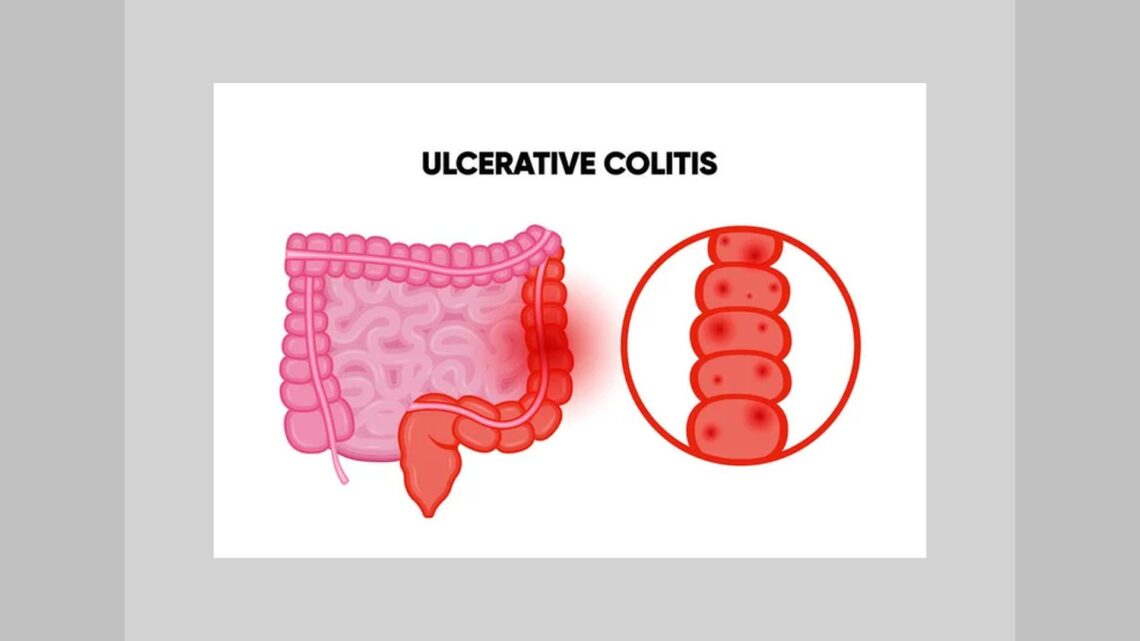
ULCERATIVE COLITIS
It is an inflammatory condition of the rectum and colon of unknown aetiology perhaps related to stress, westernized diet, autoimmune factor, familial tendency, and allergic factors.
AETIOLOGY;
- Uncertain- tendency to perforation / malignant.
- Women are more affected than males.
- Any age but in between 20-40 years more common.
- Unknown aetiology but appears to combine environmental stimuli’
- Autoimmune response and genetic factor {association with the human leucocyte antigen HLA-B27 }

PATHOLOGY-
- Unlike Crohn’s disease is mostly confined to mucosa and submucosa.
- Non-specific pathological changes are found.
- The rectum and sigmoid colon are principally affected, but the whole colon also may be involved.
EARLY CHANGES-
- Initially, there is oedema of the mucosa, with contact bleeding and petechial haemorrhage, proceeding to ulceration; the ulcers are shallow and irregular.
- Round and polymorph infiltration of the crypt of leiberkuhn at the base of mucosa forming crypt abscess.

LATER CHANGES-
- Coalescence of crypt abscesses and desquamation of overlying cells to form an ulcer.
- Undermining of adjacent relatively normal mucosa which attains Polypoid configuration due to oedema.
- Collagen and luxurious growth of granulation tissue at the area of ulceration which may extend to or even through the muscularis mucosa.
- Each bowel action drains volumes of fluid mixed with blood milked from the granulation tissue.
- Loss of haustration in the early barium enema is due to paralysis of muscularis mucosa and the ‘rigid stove pipe’ appearance of the colon later is the consequence of scarring following repeated trauma caused by bowel action.
- Ulcerative colitis is prone to developing carcinoma of the colon. Patient developing Ca. prognosis is very poor.

MALIGNANCY AND ULCERATIVE COLITIS-
- They start over the flat mucosa not in the polypoid segment.
- They are often multifocal.
- They are highly malignant and not always proliferative (hence difficult to detect especially in the rectal stump)
- Carcinoma is difficult to diagnose because symptomatology imperceptibly merges with manifestations of the original disease process more so as it may develop in mild cases where inflammation and ulceration are confined to the mucosa.

Factors promoting Carcinoma-
- Long duration of the disease.
- Total colitis is more prone to show malignancy.
- Incidence of Ca-colon is more if the first attack is severe.
DIAGNOSIS-
- Dysentery is common and is often missed.
- An acute attack is characterised by the onset of bloody diarrhoea and toxaemia with signs of prostration, hypotension and collapse.
- Perforation may follow toxic distention of the colon.
- HB% & PCV – this gives a rough idea about the replacement of blood.
- Electrolytes – In the chronic phase deficiency of ‘K’.
STRAIGHT X-RAY –
Toxic dilation of the colon
↓
An acute fulminating colitis
↓
Perforation
↓
Free gas under the diaphragm.
SIGMOIDOSCOPY & BA – ENEMA – These are also contraindicated in presence of acute attack as these investigations may precipitate perforation.

CHRONIC CASE–
- H/O diarrhoea with the passage of mucus and blood dates back,,,, months,,,,, even years…….
- Weight loss, anaemia.
- Oedema due to hypoproteinaemia → Extreme weakness because of the combination of these.
- Incidence of eye complications like iritis, skin complications like erythema nodosum and other complications like arthritis in patients with chronic diarrhoea may also help in the diagnosis.
INVESTIGATIONS-
- HB % – Anaemia ↓
- Electrolytes – K – may cause muscular hypotonia.
- Serum protein – Low especially albumin.
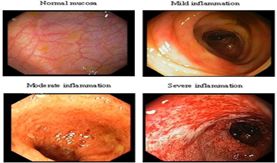
Sigmoidoscopy –
Early changes – Change in vascular pattern, and the submucous vessels are not visualised. Later changes – Granular proctitis with ulcerations at places. Crypt abscess discharging in punctuate fashion
ULCERATIVE PROCTITIS

Barium Enema – Its main advantage is to provide information regarding the extent of the disease.
It may show – ‘Tell TALE Collar Stud Projections’ indicating breach of muscularis mucosa by crypt abscess.
Loss of haustrations, and later ‘pipe
Stem Colon’.
Carcinomatous changes.
Colonoscopy – enables the whole large bowel to be inspected, the proximal extent to be noted and biopsy material to be obtained.

TREATMENT;
CONSERVATIVE – As per the surgical approach this is for the improvement of general health and is never curative, but as a homoeopath, I would claim that we have quite a good scope in treating the said condition and would succeed in curtailing the progress of the disease can also avoid the patient going towards complications or malignancy.
- High-calorie diet.
- Correction of anaemia.
- Control of diarrhoea.
- Medication
SURGICAL-
- Total Proctocolectomy with Ileostomy.
- Total Colectomy with Ileorectal Anastomosis
Homoeopathic Approach
- Merc Sol, Nux Vomica, Phosphorus, Aloe Socotrina, Ignatia, Natrum mur, Carbo Veg, Merc Cor, Nitric Acid, Lycopodium, Colchicum Autumnale, Staphysagria, Acid muriaticum, Carcinosinum
- Merc Sol — Indicated for cases of loose stools with excessive bleeding as in ulcerative colitis.
- The stools are very frequent, bowels feel weak to hold them.
- However, even after passing stool a number of times, there is no satisfaction.
- Intestines feel bruised when lying on the right side, or as if they fall to the side on which one is lying.
- Stool painful, scanty, greenish slimy, acrid stool, then tenesmus or chill, never get done feeling.
- Rectal tenesmus, with tenesmus of the bladder.
- Nux Vomica — It is useful to those persons who lead a sedentary life, doing much mental work; or to those who remain under stress and strain of prolonged office work, business cares and worries.
- One of the most useful medicines for ulcerative colitis with frequent, scanty stool and marked tenesmus.
- Tenesmus refers to the ineffectual urge to pass stool almost constantly.
- Ineffectual urging for stool and the stool is scanty.
- Abdomen pain before passing stool may be observed.
- Nux Vomica also offers great help in cases where taking spicy food or alcohol worsens symptoms.
- Craves piquant food, beer, fat food, chalk, stimulants.
- Bruised soreness of the abdominal wall.
- Strains hard at stools, feeling as if part remained unexpelled, passes small quantity at each attempt.
- Phosphorus — Phosphorus is a significant medicine for treating ulcerative colitis cases with bloody diarrhoea attended with weakness & exhausted feeling.
- The stool is copious, gushing, and watery.
- The character of the blood is bright red.
- Cramping pain in the rectum may arise on passing stool.
- Phosphorus is majorly indicated in case of inflammation of the rectum & proctitis.
- A great remedy for Crohn’s disease with characteristic symptom in the stool, which is long, slim, hard, and dry, and is evacuated with a great deal of difficulty.
- It may be compared to a dog’s stool in appearance and in manner of evacuation and is often accompanied with the same straining & trembling of the limbs.
- Stools like scraping of intestines.
- Involuntary evacuations.
- Discharge of mucus from the anus, which remains continually open.
- Aloe Socotrina — Aloe Socotrina is one of the best medicines for Crohn’s disease & ulcerative colitis with urgency to pass stool as the predominant symptom.
- The urgency to pass stool is markedly present in the morning, also soon after eating or drinking.
- There is constant bearing down in the rectum.
- Burning in the anus and rectum may be intense.
- Another characteristic feature for use of Aloes is the passage of jelly-like mucus in stool.
- Rumbling and cramp in the abdomen, before and during stool.
- Involuntary soft stool while passing wind.
- The rectum seems full of fluid which feels heavy, as if it would fall out.
- Carbo Veg — Difficult evacuations, without being hard with much straining, burning pain in the anus and pains similar to those of parturition, in the abdomen.
- Evacuations are liquid, pale or mucus-like.
- Discharges of mucus and of blood instead of faeces during the evacuation.
- Flatulent, cramp-like colic, even at night.
- Borborygmi and movements in the abdomen.
- Excessive discharge of flatus, of a putrid smell.
- Aggravation of the abdominal suffering after eating the smallest portion of food.
- The pains in the abdomen are often accompanied by anxiety and tears.
- Involuntary evacuations of substances of a putrid smell.
- Discharge of blood from the anus with every evacuation and aching pain in the abdomen.
- He cannot bear any tight clothing around his waist and abdomen.
- Merc Cor — Pain in the abdomenwith tenderness in the epigastric region and hypochondriac region, pain aggravates while lying on right side, while sensation as if something is moving inside the abdomen.
- The loose stool which is hard to evacuate bloody and slimy stool followed by faintness and trembling.
- Continuous urging to pass stool and urine.
- Stools bloody, slimy, hot with tormenting tenesmus.
- Diarrhoea is yellow, green, bilious, and bloody with membranous shreds of faeces with mucus and dark clotted blood.
- Burning in rectum and anus during stool.
- Painful bloody discharges with vomiting.
- Dysentery is corrosive, ichor, oozes from anus with the excoriating the parts.
- Itching around the anus (while walking).
- Very persistent distressing tenesmus and cutting colicky pains after stool, burning and tenesmus of rectum.
- Nitric Acid — Nitric Acid is the best choice of medicine in ulcerative colitis cases where there is intense pain in the rectum while passing stool.
- The pain may be tearing or cutting in nature.
- It may continue for hours after stool is passed.
- Profuse, bright red bleeding may be noticed along with stool in such cases.
- Tensile pressure and shootings in the hypochondrium.
- Accumulation of flatus in the abdomen.
- Borborygmi as if a boiler was working in the abdomen. (Sensation in abdomen like machinery working).
- Excessive inflation of the abdomen in the morning.
- Pain is from ulceration in the lower part of the abdomen.
- Frequent pinching and incisive pains in the abdomen.
- During stool nausea, tenesmus & spasm of the anus, cutting in the anus and rectum.
- Acute pain in the abdomen, sensation as if faeces remained and could not be expelled.
- Splinter-like pains in the rectum (with ineffectual urging), burning, tearing & palpitation of the heart.
- Sanguineous, dysenteric evacuations, with tenesmus.
- After stool-continued urging, exhaustion, irritation, anxiety, general uneasiness, with soreness in the anus, raw, cutting, straining, shooting in the rectum, continuing for hours & prolapse with the sensation of constriction in the anus with haemorrhage.
- Black, offensive blood, mucous, pseudo-membranes, with straining and burning in rectum.
- Lycopodium — Tension around the hypochondria, as from the pressure of a hoop.
- Immediately after a (light) meal the abdomen is bloated, full, and distended.
- Has a great appetite, but a small quantity of food fills him up and he feels bloated.
- Aching pains in abdomen, fullness and distension of stomach and abdomen.
- Weight in the abdomen, sensation of something heavy lying on the left side of the abdomen.
- Desire for stool followed by painful constriction of the rectum or anus.
- Small stool with the sensation as if much remained behind, followed by excessive and painful accumulations of flatulence.
- Haemorrhage from the rectum, even after a soft stool.
- Feeling of fullness in the rectum continues after a copious stool.
- Contractive pain in the perineum, after scanty, hard stool with stitches in the rectum.
- During stool burning and biting at anus, pressure, tenesmus & pain in back as if broken with haemorrhage.
Bibliography:-
- Das, Concise Text Book of Surgery 10th Edition reprinted in March 2019
- SRB’s Manual of Surgery, 6th 2019, Sriram Bhat M
- Hand Book of Surgery by S. C. Basu. 2nd Edition reprinted in 2005
- Pocket Manual Of Homoeopathic Materia Medica, Boericke William, M.D
- Clinical Materia Medica. Farrington. E.A., M.D.
- A Dictionary of practical materia medica Clarke Henry John, M.D.
- Homoeopathic Therapeutics. Samuel Lilienthal. M.D.
Dr. Jaideep Desai M.D. (Hom)
Professor & Head of Surgery,
Yenepoya Homoeopathic Medical College & Hospital, Mangalore. Karnataka.


Nitric Acid is chronic ulcerative colitis always soft stool hardly ever constipated,acrid diarrhea with tenesmus chronic hepatitis,tender pylorus enlarged congested liver,offensive stools with mucus and blood,fir like burn fissures,averse meat bread.Baehr states liver not secreting bile portal vessels compressed or wasted.Raue states old age weakness and diarrhea after typhoid fevers.Bowel nosodes explained by John Paterson should be linked.CP Bryant is expert on Nitric Acid.Podo for initial colitis stages constipate diarrhea alternate is recommended by old era homeopaths.