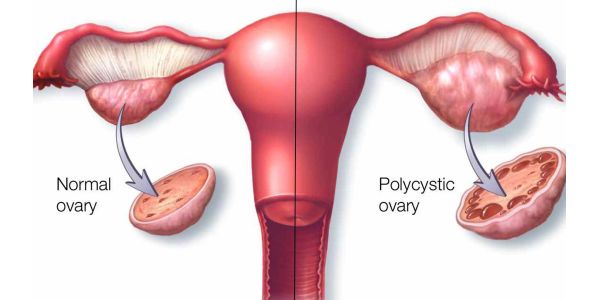
Polycystic ovarian syndrome is a heterogeneous endocrine disorder that affects one in 15 women worldwide. It is the most frequent cause of hyperandrogenism and oligo-anovulation which have substantial psychological, social and economic consequences.
It is one of the most common endocrine metabolic disorders. In a study in Indian adolescents, between 18 to 45 years, prevalence ranged from 9.31 -36% (nidhi.et.al).
Another study at Child development Centre Trivandrum Medical College, Kerala, reported 36% prevalence in adolescent girls (The Indian journal of Pediatrics, Jan 2012,vol 79)
The incidence of PCOS in the reproductive period of life is fast progressing as one of the main causes of primary as well as secondary infertility in females in the Indian scenario, leading to far reaching implications in the family and social life of the Indian community
Apart from the mental and physical frustrations due to infertility, the aesthetic changes due to the physical signs like obesity and hirsuitism together with the disturbance in the normal menstrual cycles pose intolerable untold misery and insecurity in females especially married women in the conventional Indian society leading to lack of self esteem and depression in many cases
The aetiology of the condition is unknown, but recent evidence suggests that the principle underlying the disorder is one of insulin resistance, with the resultant hyperinsulinaemia stimulating excess ovarian androgen production.
Associated with the prevalent insulin resistance, these women exhibit a characteristic dyslipidaemia and a predisposition to non-insulin dependent diabetes and cardiovascular disease in later life. Symptoms include Infertility, Abnormal menstrual cycles, obesity, hirsutism, acne, acanthosis, diabetes or insulin resistance, polycystic ovaries on USG..
Patients typically present with hirsutism in one or more of the body areas specified under the Serriman-Gallwey hirsutism scoring system. Each of the nine body areas most sensitive to androgen is assigned a score from 0 (no hair) to 4 (frankly virile), and these separate scores are summed to provide a hormonal hirsutism score.
This paper is based on Dr.Ajay Kumar’s observation of his PCOD cases for the last fifteen years in reproductive age females treated with homoeopathic medicines.
Two cases of cured polycystic ovarian syndrome in females belonging to the reproductive age group are presented below with substantial clinical data.
AIMS AND OBJECTIVES
- To ascertain the pathophysiological action of homoeopathic medicines in the treatment of polycystic ovarian syndrome in Kerala state, India.
- To create public awareness on the possibilities of Homoeopathic system of medicine in the treatment of chronic diseases permanently and without any side effects.
MATERIAL AND METHODS
A sample size of one hundred was selected from females belonging to the reproductive age group (viz. 18 to 35 years) from different districts of Kerala who approached for treatment of either menstrual irregularities, infertility, acne or obesity.
The purpose of the study was explained to the participants. Informed consent was obtained from the participants. The pre-test was conducted using a structured questionnaire to assess symptoms of PCOS and followed by diagnostic tests.. The post-test was conducted using the same structured questionnaire and diagnostic criteria after three years, from January 2012 to November 2015.
The diagnosis of PCOS was done as per Rotterdam 2003 criteria and confirmatory ultra sound scan of the pelvis depicting the polycystic profile of the ovaries. Homeopathic medicines were given based on the individualistic nature of each of the cases and cure assessed based on the clinical criteria. The diagnostic signs considered were:
ULTRA SOUND SCAN
Necklace sign in ovaries (polycystic ovaries), Ovarian volume (above 10 ml/12or more follicles of 2-9 mm),Antral follicle count, Doppler blood flow in the Ultra sound scan.
BIOCHEMICAL VALUES
Androgens (testosterone,
DHEAS), Androstenedion(LH,Progestrone,SHBG),Glucose/Insulin,Lipids
PHYSICAL SIGNS
Obesity (BMI), Hirsutism Serriman Gallway scoring system), acanthosis, acne, abnormal periods.
The effect of the drug administered was considered positive based on the following criteria
- Three consecutive normal menstrual cycles
- Positive pregnancy test in married women
- Normal ultra sound study of the pelvis in previously abnormal study (necklace sign/ovarian volume less than 10 ml/more than 10-12 follicles)
- Normal biochemical parameters compared to previous altered values
Those found pregnant after medication were discontinued treatment apart from routine pregnancy care medications for optimum health of foetus and mother
Those with normal cycles and normal biometric parameters were observed under placebo for a whole year before discontinuing treatment
ANALYSIS OF SYMPTOMS
| Total number of cases -100 | |
| Obesity | 80 |
| Infertility | 50 |
| Hirsutism | 45 |
| Acne | 35 |
| Acanthosis | 45 |
| Abnormal periods | 90 |
| Necklace sign | 54 |
| Hyperlycemia | 30 |
| Mental stress factor | 75 |
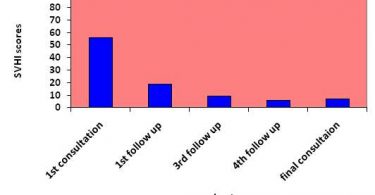
RESULTS
| Total number of cases | 100 |
| Total number of cases reported with either positive pregnancy test/normal ultra sound study of pelvis | 76 |
| Discontinued treatment | 12 |
| No result after six months treatment | 5 |
| Still under treatment with reduced BMI and variable results off and on | 7 |
Two are offered here with relevant data to manner of handling PCOS cases homoeopathically. Exhaustive inquiry into the personal history of the patient taking into account her mental generals and physical reactions to circumstances both environmental and mental are given high preference while selecting the remedy
Name: Mrs. M
Age: 21 years
Clinical presentation: Irregular periods, profuse bleeding and prolonged bleeding at onset of flow. Violent dysmenorrhoea, obesity, acanthosis in skin folds and back of neck.

FOLLOW UP
| date | Clinical symptoms | evaluation | remedy | remarks |
| 21/02/2012 | Irregular periods,BMI
30,dysmenorrhoea,joint pains |
Calcarea carb 1M | Ultra sound necklace sign | |
| 22/03/2012 | No menses,joint pains aggravation,weight increaed | Homoeopathic aggravtion | Sac lac | Waiting on medine |
| 25/04/2012 | Weight ,joint pains reduced,menses appeared
,profuse flow lasted two weeks |
amelioration | Sac lac/BT | Medicine has acted favorably |
| 26/05/2012 | No menses,color of acanthosis reduced | stagnant | Calcarea Carb 1M | Medicine exhausted action,hence repetition |
| 02/08/2012 | Menses,normal flow,6 days,BMI 25,joint pains reduced,no dysmenorrhoea | amelioration | Sac lac | Waiting on medicine |
| 06/09/2012 | Normal periods,5 days flow | amelioration | Sac lac | Medicine still acting |
| 09/10/2012 | Normal periods,slight dysmenorrhoea | amelioration | Calcarea carb 10 M | |
| 02/11/2012 | No symptoms,BMI 24 | cured | Sac lac | Cured,ultra sound scan normal |
After Treatment
DISCUSSION
This lady who came with irregular periods and episodes of anxiety was assessed based on her unique symptomatology which was typical of the drug Calcarea Carb. She was cured of her complaints in a span of one year. She was reviewed on placebo for another six months and discontinued treatment as her periods were regular during the period, and she had a normal ultra sound scan.
Case – 2
- Name : Ms. X
- Age: 21 years
- Clinical presentation: secondary amenorrhoea 4 months, irregular periods since puberty, facial hirsutism, dysmenorrhoea with chilliness from puberty. acne from puberty.
| Date | Clinical features | Totality of symptoms for prescription | Name of remedy | evaluation |
|
12/11/2012 |
Secondary amenorrhoea,
acne, hirsutism, obesity |
Plump lady with aversion to milk and fatty food, easily
weeping, mild yielding, craves open air, late puberty, dysmenorrhoea with feverish feeling at the time of menses |
Pulsattila 1M | To be evaluated after one month |
FOLLOW-UP
This case had a positive result in a remarkably short period. She was observed without medicine for another three months. Her menses was regular and there was no report of dysmenorrhoea.
Conclusion
From the data depicted, it is evident that homoeopathic drugs can play an important part in the treatment of PCOS with lasting effects. It is worth mentioning that if 76 % cure can be elicited with the use of homoeopathic drugs in conjunction with life style changes, many women have a ray of hope in infertility.
Since the approach of case taking and prescribing is highly individualistic and the same remedy cannot be used in all patients, the approach to research and its validation does not fit into the current protocols of research like blinded study or case control.
It is up to the scientific community and my fellow homoeopaths to develop a unique protocol which can unfold the vast possibilities of this simple yet sound healing art in the treatment of all diseases including PCOS, which are considered just manageable or incurable according to modern concepts of medical treatment. PCOS can be treated successfully without invasive procedures and high financial burden through the therapeutics of homeopathy.
REFERENCES
1. Marlow, R.D and A.B. Redding 2002. Textbook of paediatric nursing. 6th ed. New Delhi: Elsevier;.
2. Padubidri, G.V andN.S. Daftary,2004 Hawkins & Bourne Shaw’s textbook of gynaecology. 13th New Delhi: Elsevier;.
3. Sebanti, G., D. Rekha and S. Sibani 2005 A profile of adolescent girls with gynaecological problems. Obstet. Gynecol. India., 55(4):353-355.
4. Stankiewicz M, Norman R. 2006 Diagnosis and Management of polycystic ovary syndrome: a practical guide. Drugs.,66(7):903-12.
5. Norman, J.R., D. Deiwally., S.R Legro andE.T. Hickey,2007 Polycystic ovary syndrome. The Lancet Aug.,370(9588):685-97.
6. Puri, M and G. Sharma 2004 Insulin Sensitisers in PCOS. Obs & Gynaec Mar;9(3):181-3.
7. Pteifer, M.S and S. Kives. 2009 Polycystic ovary syndrome in the adolescent. Obstet Gynaecol Clin North Am Mar., 36(1):129-52.
8. Gagan Pcos – The Hidden epidemic Aug [online]. Available from:
URL:http://www.whereincity.com/ medical/ topic/ women-health/ articles/ 704.htm.
9. DIVFFRC (Delhi IVF Fertility Research Centre). [online]. Available from: URL:http://www.delhicom/PCOD.html.
10. The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group, 2004. Revised 2003 consensus on diagnostic criteria and long-term health risks relatedto polycystic ovary syndrome. Fertil Steril.,81: 19–25