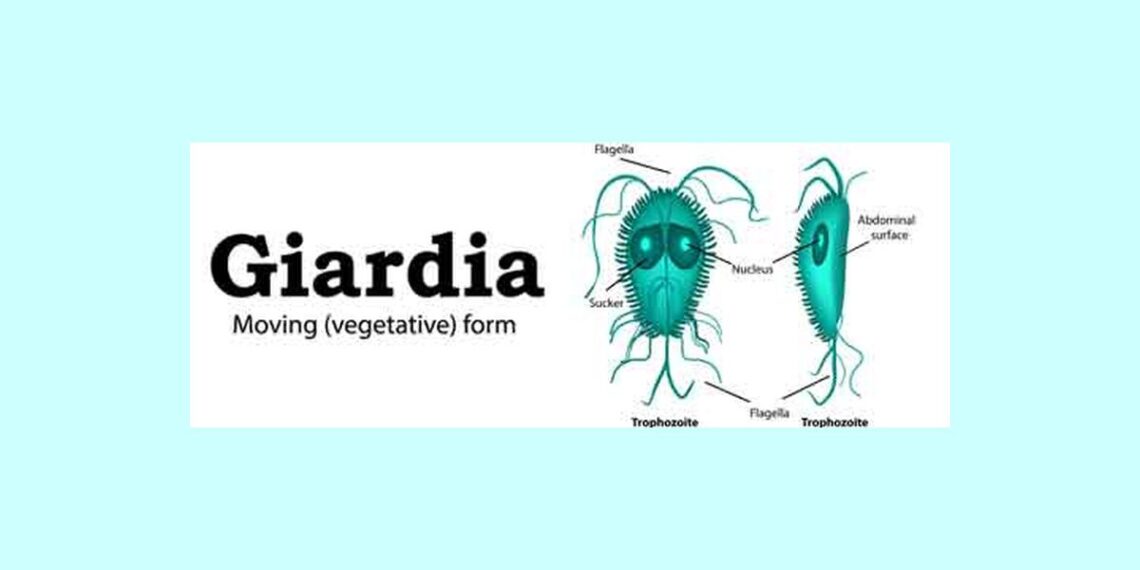
Giardiasis is an infectious disease inducing fatty diarrhea caused by the intestinal protozoa Giardia lamblia. Protozoa are single celled living organism with two cell layers: an outer layer (ectoplasm) and an inner layer (endoplasm). In cases of environment changes, the protozoa secrete a protective coat and shrink into a round, armored, infectious form called a “cyst.” When humans ingest the cyst, it transforms again into the motile form and is called “trophozoite.”
Giardiasis outbreak often occurs after sewage contamination of drinking water, or after drinking from clear mountain streams contaminated with G. lamblia. After ingestion of the cysts, the parasites transform into trophozoites in the duodenum and jejunum, and adhere to the intestinal wall. The parasites coat the duodenal and jejuna walls and interfere with fat absorption from the gut, resulting in fatty diarrhea. The parasites do not invade the intestinal wall, only coat it. The ileum is rarely affected by giardiasis.
Most patients with giardiasis are asymptomatic. Children and patients with low immunity may show mold abdominal discomfort, along with fatty diarrhea resembling celiac sprue or celiac disease diarrhea. Rarely, G. lamblia may invade the gallbladder, causing cholecystitis and jaundice. A concomitant infection with Entamoeba histolytica may be overlooked in cases of infection by large number of G. lamblia.
There is an increased incidence of giardiasis in patients with hypogammaglobulinemia. Intestinal lymphoid hyperplasia (Peyer’s patches hyperplasia) may be found in cases of giardiasis infecting a patient with hypogammaglobulinemia. Diagnosis of giardiasis is confirmed by indentifying the cysts in the stool.
The most common cause of water borne intestinal infection in the United States, giardiasis is an infection of the small intestine caused by the GIARDIA LAMBLIA protozoa, which is found in the human intestinal tract and in faces. In recent years, outbreaks of giardiasis have been common among people in institutions, preschool children, at catered affairs, and large public picnic areas.
Since the 1990s, Giardia infection has become one of the most common causes of human water-borne disease (both drinking and recreational water) the United States, Giardia are found worldwide and within every region of the United States.
Giardiasis is spread by contaminated food or water or by direct personal hand-to-mouth contact. Children can spread the infection by touching contaminated toys, changing tables, utensils, or their own feces. For this reason, the infection spreads quickly through a day-care center or institution for the developmentally disabled. Unfiltered streams or lakes that may be contaminated by human or animal feces are common sources of infection to campers
Life Cycle/Transmission of giardiasis
Giardia is one of the four common species of intestinal flagellates. It is a protozoan, single-celled parasite that exists in two forms, a motile trophozoite and cyst, with the later form causing infection. Transmitted by focally contaminated water or food, and direct person- to person contact, only 10 to 100 micro-organisms are needed to cause infection and symptoms.
Cysts multiply in the duodenum and jejunum if the human host. They reside in close approximation to the mucosa, may penetrate into the secretory mucosa, and have been isolated in the gall bladder and biliary system as well. A sucking disk located on the antral portion of ventral surface facilitates anchorage to the mucosa, akin to a sucking disk producing mechanical tissue irritation.
Pathogenesis of giardiasis
Giardia can survive in the environment because the parasite is surrounded by a thick outer coat to form a cyst (an inactive, non-feeding form). After a person or animal swallows the cysts present in contaminated food or water, the cysts break open when they reach the small intestine, releasing mature parasites does not attack intestinal cells directly.
Giardia parasites, by attaching to and covering the inner intestinal surfaces, interfere with nutrient absorption and water transport and cause diarrhea, cramps, and sometimes dehydration. As the parasites pass through the small intestines to the large intestine, they form new cysts that pass out of the body. These new cysts, if they infect other people or animals that come in contact with contaminated food or water, start another cycle of infection.
Clinical Picture of giardiasis
- Varies from symptomless cases to severe acute gastroenteritis and chronic Malabsorption. Abdominal cramps and diarrhoea are dominant features.
- Specific diagnosis cannot be based on clinical picture.
Symptoms of acute giardiasis
- Symptoms usually begin 1-3 weeks from infection.
- Epigastric cramps, nausea.
- Stools may vary from watery to more solid, and they may be profuse, foul smelling, pale and may float.
- Tenesmus is present especially in the morning and after meals.
- Bloating, flatulence, anorexia, weight loss.
Symptoms of chronic giardiasis
- Similar to the acute form but milder and periodical.
- Recurrent diarrhoea and abdominal discomfort and distension are dominant features.
Complications of Giardiasis
The following complications are possible: secondary Malabsorption, for example lactose intolerance, even subtotal villous atrophia, pancreatitis, and cholangitis rarely growth retardation in children and possibly also reactive arthritis, Urticaria and uveitis.
Diagnosis of giardiasis
- Based on detection of protozoa cysts, antigen or trophozoites.
- Stool is preserved in formalin, concentrated and microscoped for cysts.
- Usually at least three stool samples are collected 2 to 3 days apart for faecal parasite examination.
- If the laboratory test for faecal parasite is repeatedly negative, the more sensitive method of antigen detection (ELISA or immunofluorescence assay) can be used to reveal Giardia. Unlike the faecal microscopy test, antigen detection does not reveal other faecal parasite.
- Giardiasis is characterized by a so-called prepatental period, which means that protozoa may be detected in stools rather late after the transmission. Incubation period is often shorter which may lead to false negative stool samples at the onset of the disease.
- In chronic giardiasis the protozoa are few, and detection of cysts or Giardia antigens in stools is sporadic.
- Trophozoites may be searched from duodenal mucus or intestinal wash. Mucosal biopsies should be the so-called touch preps, i.e. a clean microscopic slide is touched with the villus biopsy and allowed to dry before subjecting to staining of the trophozoites.
Differential Diagnosis of giardiasis
- Other intestinal infections- finding one does not rule out another.
- Bile disorder, ulcers, gastritis, lactose intolerance
- Celiac disease, impairment of pancreatic function and other causes of Malabsorption.
Treatment of giardiasis
The two main treatment regimens for giardiasis include metronidazole 250 mg TID for 5-7 days, and Nitazoxanide 500 mg BID for 3 days.
Tinidazole and structural analog of metronidazole, is as effective as metronidazole in a single dose of 2 grams orally. In comparisons of single dose regimens, however, tinidazole is more effective. Alternates include furazolidone 100 mg QID for 7-10 days (80% efficacy).
Paromomycin, a non-absorbed amino glycoside with about 60-70% efficacy against giardiasis, may have a therapeutic role if treatment during pregnancy cannot be postponed.
Prevention of giardiasis
Contamination with Giardia may be prevented by the use of clean water supplies; the organism is able to with stand filtration and chlorination. For hiker with portable water purification system, iodine solutions are effective.
Patient teaching
- Inform patients who are receiving metronidazole (Flagyl) about the possible adverse effects of this drug, which commonly include headache, anorexia, and nausea and, less commonly, vomiting, diarrhea, and abdominal cramps. Warn against drinking alcoholic beverages because metronidazole may provoke a disulfiram like reaction. If the patient is a woman, ask if she’s pregnant because metronidazole is contraindicated during pregnancy.
- When talking to family members and other suspected contacts, emphasize the importance of stool examination for G. lamblia cysts.
- Teach good personal hygiene, particularly proper hand washing technique. Stress the need to wash hands after changing diapers or assisting children with toileting.
- Advise patients not to swim in pools or use hot tubs until 1 week after diarrhea has stooped to prevent contamination of the water, which can cause infection in others.
- Tell parents to keep their child out of daycare facilities until diarrhea is resolved.
- Recommended the use of a barrier during oral, anal sex and stress the need for hand-washing after removing a condom following anal sex or if touching the rectal area.
Homeopathic treatment of Giardiasis symptoms
Homeopathy is one of the most popular holistic systems of medicine. The selection of remedy is based upon the theory of individualization and symptoms similarity by using holistic approach. This is the only way through which a state of complete health can be regained by removing all the sign and symptoms from which the patient is suffering. The aim of homeopathy is not only to treat giardiasis but to address its underlying cause and individual susceptibility. As far as therapeutic medication is concerned, several remedies are available to cure type giardiasis symptoms that can be selected on the basis of cause, sensations and modalities of the complaints. For individualized remedy selection and treatment, the patient should consult a qualified homeopathic doctor in person. There are following remedies which are helpful in the treatment of type giardiasis symptoms:
Arsenic Album, Colchicum, Sepia, Nux vomica, Lycopodium, Sulphur, Carbo Veg, Pulsatilla, Calcaria Carb, iris V., Aloe Soc, Antim Crude, Cocculus, Ignatia, Phosphoric Acid, Rhus Tox, Abis Nigra and many other medicines.
REFERENCE
Carol Turkington, Bonnie Ashby- The Encyclopedia of infectious disease; 2007; 130
Chris A. Liacouras, David A. Piccoli- Pediatric Gastroenterology; 2007; 171-72
Marshall Cavendish Corporation- Disease and Disorders, Volume2; 2007; 381
Bllkka Kunnamo, Finska lakaresallskapet- Evidence- based medicine guide lines; 2005; 29
Robert B. Wallace- Wallace/Maxcy-Rosenau-Last Public health and preventive; 2008; 319