Keywords: Acute Pancreatitis, IrisTenax.
INTRODUCTION
Acute pancreatitis (AP) is an acute inflammatory process of the pancreas with variable involvement of other regional tissues or remote organ systems. Mild acute pancreatitis consists of minimal or no organ dysfunction and an uneventful recovery. Severe pancreatitis manifests as organ failure and/or local complications such as necrosis, abscess, or pseudocyst. Overall, about 20%of patients with acute pancreatitis have a severe course, and 10% to 30% of those with severe acute pancreatitis die.
INCIDENCE
Male: female ratio is 1:3 in those with gallstones and 6:1 in those with alcoholism.
AETIOLOGY
Non–traumatic(75%)
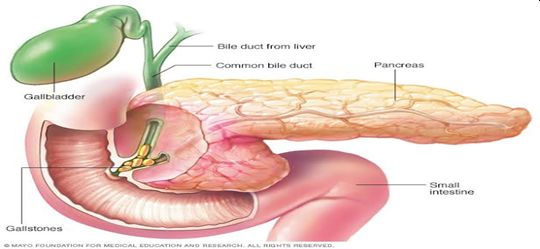
- Biliary tract diseases
- Alcohol
- Viral infections (EBV,CMV,mumps)
- Drugs (Steroid,thiazide)
- Scorpion bites
- Hyperlipidemia
- Hyperparathyroidsim
Traumatic(5%)
Idiopathic(20%)
PATHOLOGY
INITIATING PHASE
-Activation of the intra pancreatic digestive enzymes
– Acinar cell injury, it acts as inflammatory and the injured cells generate cytokines and chemokines
PERPETUATING PHASE
-Events perpetuating inflammation involves recruitment of leucocyte
– Neutrophils, lymphocytes and monocytes escalate the local inflammation
THIRD STAGE
-Proteolysis, oedema, interstitial haemorrhage, necrosis
CLINICAL FEATURES
The most common symptoms and signs include:
- Severe abdominal pain (mostly over the epigastric region) radiating to back.
- Nausea
- Vomiting
- Loss of appetite
- Generalised weakness
- Fever
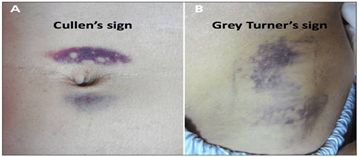
Signs which are less common and indicates severe disease, include (Inspection)
- Grey-Turner’s sign (Hemorrhagic discolouration of the flanks)
- Cullen’s sign (Hemorrhagic discolouration of the umbilicus.1
- P/A – ON Palpation
- Muscle guarding present
- Tenderness
CASE
PRELIMINARY DATA
Name : MRS.F A
Age: 22 Years
Sex: Female
Education: PUC Occupation: House wife Religion: Islam
Marital Status: Married
Date and Time of admission: 13-06-2019 at 6:15PM
IP NO: 1007094
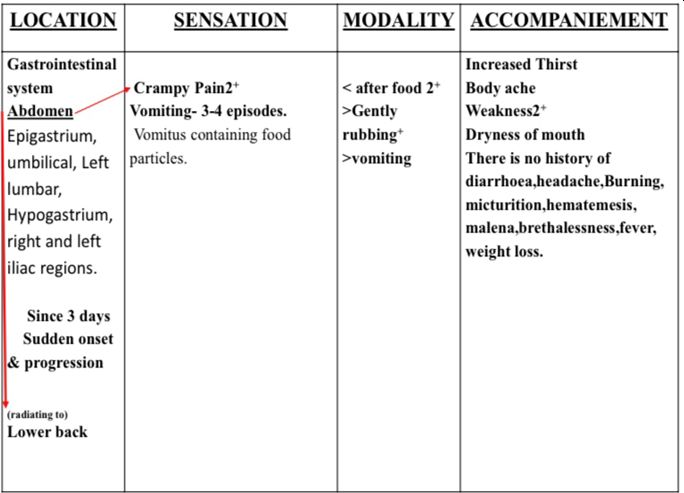
CHIEF COMPLAINT
Patient presented with the complaints of abdominal pain and vomiting for the last 3 days.
Past Medical History: Chickenpox 15 years of age.
Past Treatment History: Allopathic Medication for the same.
Past Surgical History: Appendicectomy done 5 years back.
Family History: Mother: Type II DM And Hypertensive 7/29/2020.
Personal History
▪ Diet: Mixed; Appetite: Good.
▪ Thirst: Half Litre Per day but increased since 3 days.
▪ Craving: Spicy food 2+; Aversion: vegetables2+
▪ Bowel habits: once/ day. Bladder habit: 4- 5times/day, 2times at night, no difficulty. Perspiration: Generalised
▪ Sleep: Good. Dreams: unremembered
▪ Thermal: Hot patient
MenstrualHistory
- FMP: 12 years; LMP: 27/5/2019 (Regular cycle, 6 days flow, 2 pads/day).
ObstetricalHistory: G0 P0 L0 A0 D0
General Physical Examination
- Well oriented with time, place and person.
- Moderately built and nourished.
- No signs of pallor, cyanosis, clubbing, icterus, oedema and lymphadenopathy.
Vital-signs
- Temperature: Afebrile at the time of examination
- P: 110/80mmHg ;
- Pulse: 90/minute;
- Spo2 : 99%
- Weight :48kg
Per abdominal Examination
- Inspection: Surgical scar marks present over the right iliac area.
- Palpation: Tenderness over the epigastrium, umbilical, left lumbar, hypogastrium, right and left iliac regions.
- Muscle guarding present.
INVESTIGATIONS DONE ON 13-06-2019
- Total Leukocyte Count: 19.24*10^3/μL
- Neutrophil: 75.6%
- Lymphocyte: 16.4%
2. USG- Abdomen: Partially distended gall bladder.
- Impression: No sonological abnormality detected.
3. Urine analysis: Normal
4.Serum Amylase : 140 IU/L
SPECIFIC MANAGEMENT
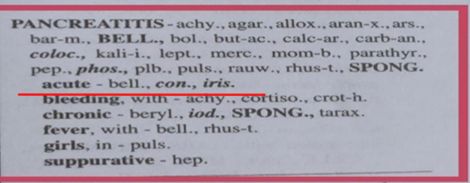
Robin Murphy- Homoeopathic medical repertory
CHAPTER:
GLANDS/CLINICAL
RUBRIC:
PANCREATITIS
SUB RUBRIC :
ACUTE
REMEDIES:
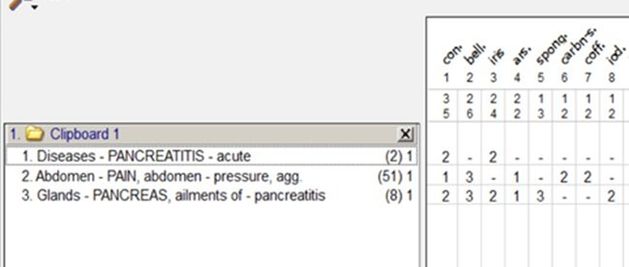
Bell, con, iris 2
REPERTORIAL RESULT
13/06/19 at 6 pm – Medicine Prescribed
Rx;
- IRIS TENAX 6 (1 packet /4th hourly)
- MAG PHOS 6X for pain
13/16/19 at 8pm
- C/o 2 episodes of vomiting after food
- Nausea present
- Pain abdomen persisting
Rx
1.IVF –RL 1 POINT 75 ml/hr
2.Continue the same treatment.
14/06/19 at 8:45 AM
- c/o Abdominal pain better
- c/o Weakness better
- c/o Nausea better; No new episodes of vomiting
- Appetite: good
- Thirst: good
- Bowels and bladder habits: Good
- Sleep: Good
- O/E : P/A : – Tenderness and guarding reduced
Investigations CBC advised
Rx
- IRIS TENAX 6 ( 1 packet /4 hourly)
- MAG PHOS 6X for pain
14-06-2019
- COMPLETE BLOOD COUNT
- HB:12.2 G%
- Total Count : 9800/cmm
- Neutrophils : 68%
- Lymphocytes: 27%
- ESR : 50 mm/1st Hour
15/06/19 at 8:45 AM
- C/o Pain abdomen reduced
- C/o Weakness reduced
- No nausea; No new episodes of vomiting
- Appetite: good
- Thirst: good
- Bowels and bladder habits : good
- Sleep: refreshed
- O/E –No tenderness over abdomen
Rx
- IRIS TENAX 6 (1 packet /4 hourly)
- MAG PHOS 6X for pain
iii. Advised SERUM AMYLASE
- 15-06-2019
Serum Amylase : 80 IU/L
- 15-06-2019 : Patient discharged with following medications and diet
Rx;
- IRIS TENAX 6 (1-1-1) for 1 week
2..MAG PHOS 6X for pain
3.Avoid Non veg and oily foods.
4.Review on 24-06-2019 on Medicine OPD.
FOLLOW UP ON 24-06-2019
- C/o Pain abdomen reduced
- C/o Weakness reduced
- No nausea; No new episodes of vomiting
- Appetite: good
- Thirst: good
- Bowels and bladder habits: Good
- Sleep: Refreshed
- O/E –No Tenderness over abdomen
No new complaints. Generally good.
Rx,
1.Mag phos 6x – 2 tablets (S.O.S for pain) for 1 week.
2.Avoid oily and fatty foods.
CONCLUSION
This is a case of 22 years old female who presented with acute abdomen and was diagnosed as acute pancreatitis. The specific remedy was Iris Tenax 6.
REFERENCE
1.Y.P Munjal; API Text Book of Medicine; Page no: 813;9th edition; Jaypee Brothers Medical Publishers (P) Ltd.
2.N.D Robin Murphy; Homoeopathic Medical Repertory;3rd Revised Edition; B-Jain large print (P) Ltd.