


Gilbert’s syndrome (GS), a neglected disease of modern health science is usually harmless, but can sometimes harm an individual seriously.
Gilbert’s syndrome is a common genetic hepatic disorder, caused by the inheritance of an abnormal gene, i.e. UGT1A1, characterized by elevated levels of unconjugated bilirubin in the blood stream, due to the reduced activity of the enzyme glucuronyltransferase, responsible for the conjugation of the bilirubin and a number of other lipophilic molecules along with several drugs also. Gilbert’s syndrome is more common in males than females and more in stressed persons. We know that changes in the UGT1A1 gene causes this potentially benign inherited hepatic disorder, and that UGT1A1 provides instructions for making the bilirubin uridine diphosphate glucuronyltransferase (Bilirubin-UGT) enzyme, found primarily on the liver cells. The bilirubin-UGT performs a chemical reaction essential for detoxification, called glucuronidation. During this reaction, the enzyme transfers glucuronic acid to unconjugated bilirubin and finally that to conjugated bilirubin. The principal actionof glucuronidation is to make substances water soluble for removal purposes.
Gilbert’s syndrome occurs worldwide but some mutations occur more often in particular populations. In many populations, the most common genetic change that results into GS is known as UGT1A1*28 and occurs in the promoter region, which controls the production of the bilirubin-UGT. This genetic change impairs enzyme production. However, this change is uncommon in Asian populations and affected Asians often have a mutation that changes a single protein building block in the bilirubin-UGT enzyme. This type of mutation, known as the missense mutation, resulting in reduced enzymatic function. Now come to the topic pathophysiology of GS. Uridine diphosphoglucuronate transferase (UDPGT) is the enzyme responsible for conjugating bilirubin into bilirubin monoglucuronide and bilirubin diglucuronide; it is therefore the rate-limiting step of bilirubin conjugation.

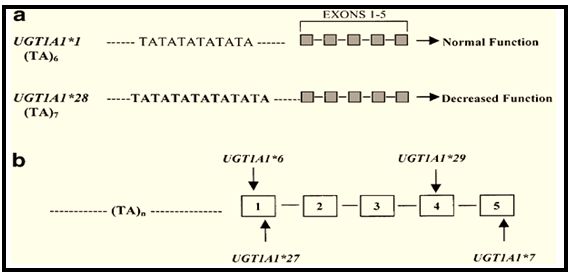
This occurs in the endoplasmic reticulum of hepatocytes. There are 5 exons that ultimately lead to production of uridine diphosphoglucuronate. Exon 1 determines substrate specificity. Among the 13 different types of exon 1, Exon 1a encodes variable region for UDPGT-1A1, the enzyme responsible for conjugation of bilirubin. Upstream to exon 1a, there is a TATAA box promoter region, normal sequence of which is A[TA]6TAA. Page no. 01
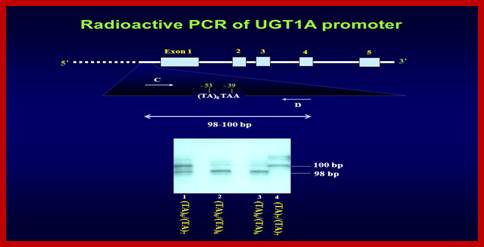
But the people with Gilbert’s syndrome inherit a different sequence of the promoter region, i.e. A[TA]7TAA.
Other mutations have been discovered within the coding regions of the UDPGT-1A1, leading to the Gilbert’s phenotype. There is some evidence suggesting that the patients with UDPGT-1A1*28 may have abnormal metabolism of protease inhibitor which leads to deficiency in the endogenous protease inhibitor, like α1- antitrypsin, which may lead to several diseases affecting respiratory system, hepato- biliary system and gastro-intestinal system in varying degree. There is also evidence suggesting that these mutations provide a protective effect in the development of Hodgkin’s lymphoma and cardio-vascular disorders.
The question arises, what are the influences of this abnormal mutation? There is no answer found regarding this question. However, I will try to postulate the probable influencing factors briefly. To undergo mutation, DNA needs to go through the ‘break and repair mechanism’ influenced by several endogenous and exogenous factors. To continue the discussion in details we should offer a snapshot about the UGT1A1 gene.

The uridine diphosphate glucuronyltransferase (UGT) enzymes are a superfamily of enzymes responsible for the glucuronidation of target substances. The transfer of glucuronic acid renders xenobiotics and other endogenous compounds water soluble, allowing for their biliary or renal elimination. The UGT family is responsible for the glucuronidation of many compounds, including hormones, flavonoids and environmental mutagens. Liver is the site where most of the members of UGT family are principally expressed, as well as in other tissues also such as intestinal, gastric or breast tissues. One of the transcripts encoded by the UGT1A locus is UGT1A1, which is at the furthest 3’ end of the UGT1A exon 1 region. UGT1A1 is expressed hepatically, as well as within the colon, intestine and stomach. Main functions of UGT1A1 lies within the liver, where it is the sole enzyme responsible for the metabolism of bilirubin, the hydrophobic breakdown product of ‘haem’ catabolism. UGT1A1 alleles have also been associated with the development of various cancers. Along with bilirubin and pharmaceuticals, UGT1A1 enzyme have been seen to glucuronidate Benzo () pyrene-trans-7, 8-dehydradiol, a precursor to the potent carcinogen Benzo (α) pyrene-7, 8- dehydradiol- 9,10- epoxide, found in charbroiled food, coal tar and cigarette smoke. They have also been noted to glucuronidate oestradiol, as well as 2- amino- 1- methyl- 6- phenylimidazo (4, 5) pyrene (PhIP), another carcinogen present in cooked meat. UGT1A1 therefore exhibits a protective effect against benzo (α) pyrene & PhIP mediated carcinogenicity and modulates the level of oestradiol within the body.
The *28 allele has been shown to increase the risk of developing colorectal cancer and breast cancer across multiple studies in Chinese and Asian populations. There is also evidence suggesting that UGT1A1*28 allele may offer protection from cardio-vascular disorders. Bilirubin is a known antioxidant and is capable of preventing plaque formation, leading to atherosclerosis. Multiple studies have found a link between low bilirubin concentrations and an increased risk of cardio-vascular disease, though this association may be affected by cofounders, such as obesity or hypercholesterolaemia. This is about UGT1A1 gene in short
For mutation, it needs to under the ‘damage and repair mechanism’ of DNA repeatedly, so, from this point of view it is clear to us that there might be some influences, which provoke the DNA for this damage and repair procedure, resulted into this mutation. Now the next question is what are the influences? Purpose of this damage and repair mechanism of DNA is to modulate themselves according to the concerned atmosphere for the purpose of avoiding the harmful effects of those atmospheres. We can say easily from the previous part of our discussion that the probable causes of the mutation are——
- The ancestors of the particular patient were exposed to excessive stress, which may results into oxidative damage to the tissues dangerously; due to which, level of dopamine, aldosterone, cortisol and other anti- stress hormones are elevated in considerable amount within the blood. For that reason bilirubin concentration in the blood become elevated, as bilirubin exhibits an anti-oxidant property; or
- 2) the ancestors suffered from the diseases, which can be prevented by the help of this mutation.
So, we can see from this discussion that UGT1A1*28 mutation reveals a long continued suffering of not only a patient, rather his or ancestors also.
Now, come to the part, i.e. clinical presentation of the patients with Gilbert’s syndrome, generally complicated with other disorders, like haemolytic anaemia, fatty liver, gastro-oesophageal reflux disorder, irritable bowel syndrome and some neurological disturbances:
| Sr. No. | Known, Effects | Symptoms |
| 01 |
Functional disturbance of liver |
· Chemical sensitivity
· Excessive allergic reactions · Drug intolerance · Toxic feeling |
| 02 |
Gastroparesis |
· Nausea ⇒ Vomiting, Decreased appetite ⇒ Easily satiety ⇒ Loss of appetite
· Abdominal bloating/Flatulence · Heartburn · Gastro-oesophageal reflux disorder · Indigestion · Hypoglycaemia · Loss of appetite ⇒ Weight loss⇒ Low body weight |
| 03 | Essential tremor | · Tremor/Trembling of hand |
| 04 |
Hyperbilirubinaemia |
· Jaundiced eyes, i.e. yellowish discolouration of the upper bulbar conjunctiva ⇒ Itchiness in the eyes.
· Jaundice ⇒ Itchiness · High coloured urine · Clay coloured stool · Excessive anger |
| 05 |
Hepatic enlargement/ Swollen liver |
· Pain and tenderness in right hypochondrium
· Pain in the region of Gall bladder · Dull abdominal pain |
| 06 |
Immune suppression |
· Catches cold easily
· Easily affected by diseases |
| 07 | Gall stones/ Cholelithiasis/ Cholecystitis | · Light coloured stool
· High coloured urine · Jaundice · Itching · Abdominal pain · Nausea · Vomiting · Back pain · Abdominal bloating · Fatty food intolerance · Sweating |
| 08 |
Hypothyroidism |
· Fatigue
· Tiredness · Depression · Dry skin · Cold hands & feet · Chilliness · Irregular bowel habit · Constipation · Poor memory · Deficient concentration · Anxiety · Dysphagia · Low body temperature · Lump in the throat · Feeling of anti- social · Pain in joints · Mood swing · Environmental allergies · Pain in eyes · Sinusitis · Light sensitivity · Dizziness · Headache · Night sweat |
| 09 |
Chronic Fatigue Syndrome |
· Fatigue
· Myalgia · Brain-fag · Gastro-intestinal disturbances · Headaches · Sore throat · Insomnia · Low body temperature · Chest pain · Sinus pain · Rhinitis · Back pain · Loose stools |
| 10 |
Candida |
· Food intolerance
· Headache · Brain-fag · Myalgia · Joint pain · Sinusitis · Fatigue · Allergies · Chemical sensitivity · Irregular bowel disorder · Mood swings · Numbness and tingling in extremities · Night sweat · Gastro- intestinal disturbances · Irritability · Anger · Poor memory · Chest pain · Dizziness |
Homoeopathic treatment of Gilbert’s syndrome
At first I am going to discuss, a case of Gilbert’s syndrome that came to me. Other cases also had a similar outcome.
CASE
| PATIENT’S DETAIL |
| NAME: XXXXXXXX
AGE: 42 Years SEX: Male OCCUPATION: Employee at Eastern Railways ADDRESS: Garia, Kolkata MARIETAL STATUS Married |
| PRESENT COMPLAINS IN DETAIL |
| 1. Feeling of an unexplainable uneasiness in the abdomen.
2. Irregular bowel habit, generally constipated, hard ball like stool with constricted feeling in anus. 3. Vertigo, tendency to falling on sides. 4. Bloody stool with burning in rectum and pain reappears with every effort. |
| HISTORY OF PAST ILLNESS |
| · Jaundice at the age of 1 year 6 months with Haemolytic anaemia
· Jaundice at the age of 8 years 3 months with acute gastro- enteritis · Jaundice at the age of 19 years · Jaundice at the age of 35 years · History of continuous elevation of the bilirubin level in the blood. |
| FAMILY HISTORY |
| · Paternal History-
Father is a patient of Gilbert’s syndrome, Decompensated Liver Disorder, HTN, Haemorrhoides. Paternal grandfather is died in CVA was a patient of Gilbert’s syndrome. · Maternal History– Mother is a patient of Diabetes mellitus- II, Fatty liver Maternal grandfather was a patient of Dyslipidaemia, Coronary artery disease and Diabetes mellitus- II. Maternal grandmother was a patient of Fatty liver, fatty degeneration of heart. |
| PHYSICAL GENERALITIES |
| Thermal reaction- Ambithermic patient
Appetite- Diminished, but cannot tolerate hunger. Every food Causes distress in the stomach. Desire- Lukewarm food, Meat, Alcohol, Pungent, Fried foods Aversion- Simple foods Intolerance- Empty stomach, Milk, Tight clothing, Excessive heat or Cold, Hot drinks. Thirst- for large draughts, but at long interval. Addiction- Smoking, Alcohol Stool- Constipated, hard ball like, constricted feeling in the Anus, very offensive smell, black in colour, ineffectual desire Urine- Yellowish, with constricted feeling in the urethra. Sweat- Profuse perspiration, sensation of hot perspiration, with offensive smell. Sleep- Sleepiness in entire day but cannot sleep, because all the complains are aggravated in sleep. Dream- of snake, fire, dead bodies, amorous matters. General tendency- of gum bleeding, small wound bleed profusely, Sleep into aggravation. |
| MENTAL GENERALITIES |
| 1. Great loquacity, talkative,
2. Selfish, , no desire to mix with the world 3. Mental labour best performed at night. 4. Averse to business 5. Loves travelling 6. Time sense deranged. |
| PROVISIONAL DIAGNOSIS |
| Fatty Liver
Gilbert’s syndrome |
| LABORATORY INVESTIGATIONS |
| 1. Blood for C.B.C., L.F.T., Lipid profile.
2. OBT stool |
| LABORATORY FINDINGS |
| Haemoglobin: 5.6 gm/dl
Erythrocytes (RBC): 2.27 millions/cu PCV%: 16.6% MCV: 75.1 fL MCH: 24.0 pg MCHC: 27.2 % Platelet Count: 0.60 lakhs/ cu mm TLC: 9.00 thousand / cu mm TOTAL BILIRUBIN 2.34 mg/dl DIRECT BILIRUBIN 0.60 mg/dl INDIRECT BILIRUBIN 0.64 mg/dl SGOT 45 U/L SGPT 65U/L ALKALINE PHOSPHATASE 677 U/L TOTAL PROTEIN 5.0 g/dL STOOL FOR OBT +ve |
| CONFIRMED DIAGNOSIS |
| Gilbert’s syndrome with hepatic dysfunction |
| SELECTION OF THE MEDICINE |
| Ø Lachesis 0/1
1 6 dosages in distilled water O.D. X 16 days in morning on empty stomach. Ø Carduus marianus Q 10 drops X B.D. X 20 days In addition, ask the patient to come after 16 days with OBT Stool. |
| FOLLOW UP |
| After 16 days,
1. Uneasiness in the abdomen relieved. 2. Vertigo disappeared. 3. OBT stool: -ve 4. Bowel habits became regularized. |
| FOLLOW UP PRESCRIPTION |
| Ø Lachesis 0/2
16 dosages in distilled water O.D. X 16 days in morning on empty stomach. Ø Carduus marianus Q 10 drops X B.D. X 20 days. In addition, ask the patient to come after 16 days with following reports, i.e. Hb%, L.F.T. |
| SECOND FOLLOW UP |
| No complain
Blood Reports: Haemoglobin: 13.0 gm/dl TOTAL BILIRUBIN 0.45 mg/dl DIRECT BILIRUBIN 0.12 mg/dl INDIRECT BILIRUBIN 0.52 mg/dl SGOT 14U/L SGPT 17U/L ALKALINE PHOSPHATASE 110 U/L TOTAL PROTEIN 6.8 g/dL |
| PRESCRIPTION |
| All the medicines are stopped and I asked the patient to come back after 4 months with the previously prescribed investigations. |
| FINAL OUTCOME |
| No abnormality is detected. |
Now what is the basis of selection of the simillimum? Lachesis is the diluted poison of the snake Surukuku, which is a haemotoxin, composed of several chemicals, like phospholipase A2, lysophospholipase, metalloprotease etc which may result in severe haemorrhage, gastro-intestinal disturbance, urinary suppression, hepatic dysfunction etc, but when administered in a well indicated case as a homoeopathic remedy can establish a cure. Because when administered in a diluted form it produces those effects which are produced by the toxin in crude state, but in less intensity and as per “Nature’s law of cure”, the desired curative effect is established.
So, from the above discussion we can draw a conclusion very easily, i.e. although GS is a benign condition, its mutation is not yet negligible and even this condition may result in several fatal conditions. A perfect simillimum is able to cure such a case.
Reference:
https://www.pharmgkb.org/gene/PA420?tabType=tabVip
http://www.gilbertssyndrome.com/symptoms.php
https://link.springer.com/chapter/10.1007/978-1-4899-0703-5_11#page-1
https://www.omim.org/entry/191740
https://en.wikipedia.org/wiki/Detoxification_(alternative_medicine)
https://en.wikipedia.org/wiki/Efflux_(microbiology)
http://www.lifeextension.com/protocols/metabolic-health/metabolic-detoxification/Page-01
http://www.jbc.org/content/289/35/24020.full
https://en.wikipedia.org/wiki/TATA_box
http://www.namrata.co/uronic-acid-pathway/
https://www.slideshare.net/preethinairtvm/biotransformation-15847897
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2729330/
http://www.malacards.org/card/gilbert_syndrome
http://www.wjgnet.com/1948-5182/full/v4/i2/18.htm
https://www.ncbi.nlm.nih.gov/pubmed/3402702?dopt=Abstract
http://www.gilbertssyndrome.com/
http://www.futuremedicine.com/doi/abs/10.2217/bmm.12.4?journalCode=bmm
http://molgendia.com/ugt1a128—genotypowanie-zest.html
https://ghr.nlm.nih.gov/condition/gilbert-syndrome#inheritance
http://bestpractice.bmj.com/best-practice/monograph/346/basics/pathophysiology.html
http://www.dovemed.com/diseases-conditions/gilbert-syndrome/
https://en.wikipedia.org/wiki/Gilbert%27s_syndrome#Notable_cases
http://www.nhs.uk/conditions/gilbertssyndrome/Pages/Introduction.aspx
Harrison’s Internal Medicine
Clinical medicine by Kumar & Clarke
Medicine by Cecil
Clinical Repertory, Dr. Robin Murphy
Materia Medica, William Boericke
A Dictionary of Practical Materia Medica, John Henry Clarke.



Wonderful presentation of a rare disease in an unique scientific manner. Why should not you arrange some seminars with this author.
Excellent scientific presentation. You could discover more mental / Gen symptoms of Lachesis Muta in your case taking. Doctor, don’t you think that Lachesis itself was enough to cure the case 100% ?
Thanks for this nice case presentation.
I dont understand that…. I m siffering from GS i simply want know is there any treatment for this……
I am suffering Filbert Syndrome , My blood result showing brilliantine colour 3.2 . can you suggest medicine?
I am suffering Gilbert Syndrome , My blood result showing brilliantine colour 3.2 . can you suggest medicine?
I wanna contact for the same issue..