Abstract:
Homeopathic Intervention in surgical disorder is challenging because the objective of the treatment is to replace the need of antibiotics and surgical knife without the removal of disease tissue and heal the individual. Surgeons will often treat by performing the excision of the disease tissues and administering the antibiotics for infection control.
Keywords: Infective cellulitis, Latent diabetes mellitus, Mental behavioural symptom, One sided disease, Local maladies, Primary surgical disease, Secondary surgical disease, Tubercular Miasm, Latent psora, Boger’s approach
Introduction: Surgical diseases are often considered as local diseases where there is local manifestation of the generalised or localised disease phenomenon. In either way the entire individual is diseased. Modern medicine would advise the local excision or removal of the affected infected part which in no way alters the disease process established in the individual body.
The only purpose of it is to reduce the disease load or reduce the risk of future or impending septicaemia. The same can be achieved without the surgical excision, only with the help of the perfect indicated homeopathic remedy.
CASE:
A 60-year-old female patient who was a known case of hypertension and hypothyroidism presented with painful oedema of left foot which had purplish discoloration and pus pockets.
Fig 1: Photo of left foot infective cellulitis

INVESTIGATIONS: 4/7/19
| Hb : 12.6
|
WBC : 13200
|
Platelet 251000
|
| HbA1C 5.5
|
Blood Sugar levels on Glucometer: 274 mg/dL
|
Fasting Blood Sugar 114 mg/dl |
| S.Creatinine 0.7mg/dl
|
S.Electrolytes: Sodium: 139 mEq/L
Potassium: 4.2 mEq/L Chloride: 104 mEq/L
|
Urine Routine: pus cells 6-8/hpf
|
| Fig 2 X ray foot left AP and Oblique, there is no osteomyelitis. |
| LOCATION | SENSATION | MODALITIES | Mental concomitant |
| Left foot
Since 3 days
|
§ Started with itching in foot – swelling – vesicles
§ Discharging watery fluid with bright red bleeding few drops (sero-sanguinous discharge ) § Burning 3+ § Throbbing3+ pulsating pain § Erythema with purple discoloration No fever No lymphadenopathy |
A/F: feet getting wet (?)
> Cold fomentation3+ >Pressure < night |
Hurriedness 3+ |
Disease Understanding:
Cellulitis: It is an acute inflammatory condition of skin characterized by local erythema, pain, swelling and heat Due to any type of injury. Frequently associated with lymphangitis and fever. [5]
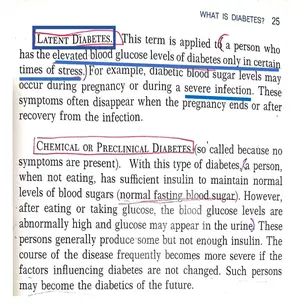
| Fig 3. Joslins Manual on Diabetes [4] |
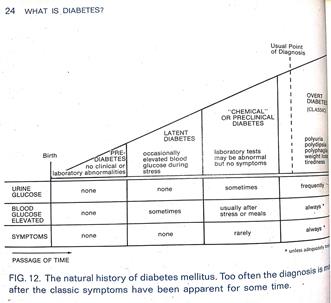
| Fig 4. Joslins Manual on Diabetes [4] |

DIAGNOSIS: INFECTIVE CELLULITIS of LEFT foot with Blister Formation
with Latent Diabetes.
CAUTION:
If patient is not treated at this point patient can have complications such as necrotizing fasciitis & osteomyelitis.
CLASSIFICATION OF DISEASE:
Dynamic Acute Surgical Individual Disease with ONE SIDED PRESENTATION
ONE SIDED PRESENTATION as explained by the following aphorisms
Aphorism 173
The only diseases– have– few symptoms, termed one-sided, because they display only one or two principal symptoms which obscure almost all the others.
Aphorism 177
In order to meet most successfully such a case as this, which is of very rare occurrence, we are in the first place to select, guided by these few symptoms, the medicine which in our judgment is the most homoeopathically indicated.
Aphorism 185
Local diseases – so called – not just the local part – but the individual is affected as a WHOLE
Even though local part is infected ( the left foot) there is increased WBC count & blood sugar levels indicating the involvement of the whole individual. [1]
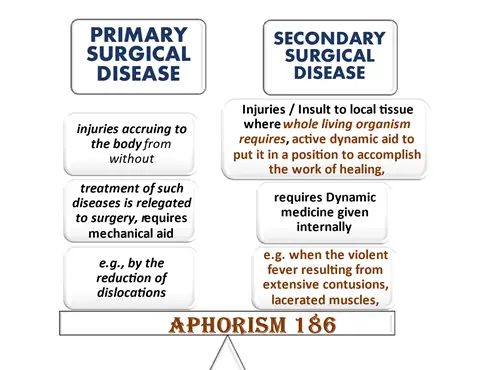
| Fig 5. Figure representation of Aphorism 186 |
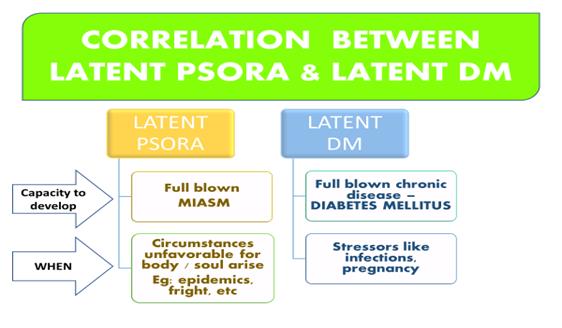
| Fig 6. Representation of correlation between latent diabetes & latent psora |
According to Aphorism 194, The acute disease is a product of psora which had hitherto remained latent in the interior, but has now burst forth and is on the point of developing into a palpable chronic disease.
MIASMATIC DIAGNOSIS: TUBERCULAR
- Hurriedness at mental and physical level
- rapid progress
- A/f – damp weather
- Indolent system with hypertrophic changes
- Increased activity leading to debility
- Stimulation of R. E. S
- Hyperdynamic changeable w.r.t emotions, intellect, desires, response
- Diabetic syndrome
- Hyperactivity with debility
- In turn causes subject to be more vulnerable to infections esp. Tuberculosis
- Giving rise to inflammation of serous membranes, subcutaneous tissues [9]
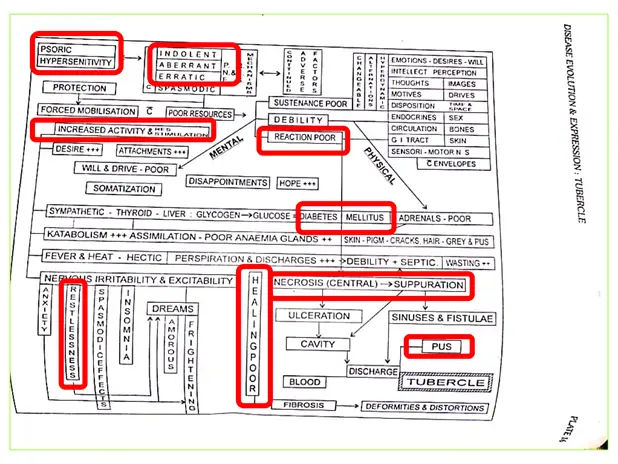
| Fig 7. Disease evolution & expression of tubercle – ICR SYMPOSIUM VOLUME C |
Evaluation of case:
- Susceptibility: low
- Few symptoms at level of physical particulars and mentals
- Old age
- Trivial injury/exposure leading to Infective cellulitis
- One sided presentation
- Paucity of symptoms
- With not much qualified physical generals or mentals
Totality of symptoms using Boger’s approach:
- Gen: Wet agg
- Gen: Cellulitis
- Gen: Cold amel
- Mind: Hurry haste tendency
- Extremity pain: burning
- Extremity pain: pulsating
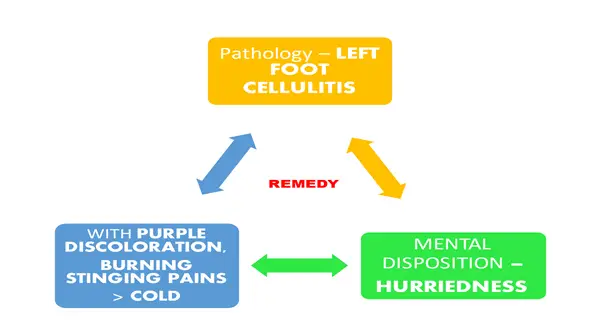
| Fig 8. Representation of Totality of Symptoms |
Remedy Differentiation: –
| ARSENIC ALBUM | TARENTULA CUBENSIS | LACHESIS | LEDUM PAL | |
| Sensation | Old ulcers with burning & lancinations | Atrocious burning or sharp stinging pains
Pungent heat of surface |
Burning in spots
Sn as if hot air were passing |
Throbbing pains
Ascending type of rheumatism |
| Local symptoms | Swelling of foot hard & shiny
Burning vesicles of blue black color |
Hard & indurated abscesses & carbuncles
Bluish purple discoloration |
Flat ulcers or swellings with blue/ purple surroundings | Edematous Swelling, ecchymosis, black blue discoloration.
Punctured wounds |
| Side affection | Right sided | Left sided | Left sided | Left shoulder & right hip |
| Causation
and Modalities |
< Bathing , straining ,
< Grief, fright > Heat < cold |
< getting wet
< night |
Injuries,
< heat < grief , vexation |
Puncture wounds
< night < warmth > cold |
| MIND | ANGUISH
RESTLESSNESS Cant sit in a place |
Nervous restlessness
Hurry Haste |
Insupportable anxiety
indolence with dislike for any labor |
Anger
Dissatisfied, hates & avoids company |
MATERIA MEDICA REFERENCES:
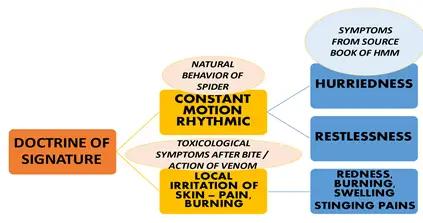
Bogers Synoptic Key states that in Tarentula the seat of disease is cellular tissue. Onset of the disease is rapid with alarming prostration, atrocious burning or sharp stinging pains, sepsis, fidgety, purple discoloration, pungent heat of the surface.
Robin Murphys repertory mentions in the chapter Generalities “Cold Amel” Tarentula H. and Tarentula Cubensis remedies.
John Henry Clarke states: abscesses ending by mortification of the integuments over it, and having small openings, discharging a thick, sanguinous matter containing pieces of mortified cellular tissue, fasciae and tendons.
Phatak’s Materia medica states that Tarentula cubensis is toxaemic medicine useful for septic conditions, atrocious burning, bluish abscesses, Bluish abscesses, painful abscesses,
Boericke’s Materia medica states that Tarnetula Cubensis has septic condition, malignant suppuration, purplish hue and burning stinging pains.
| Fig 17. Boericle materia medica [7] |
| Fig 9. Doctrine of signature of Tarentula Cubensis Spider |
REMEDY PRESCRIBED:
- TARENTULA CUBENSIS 200, half hourly.
| FOLLOW
UP |
SYMPTOMATIC | ON EXAMINATION | Rx |
| DAY 2 | q Pain and heaviness in left foot reduced
q Burning and stinging decreased |
q Oozing of fluid and blood reduced
q Tenderness mild q Edema present but erythema reduced q HGT: 175 mg/dl |
Tarentula cubensis 200,
2 hourly |
| DAY 5 | q Pain only on touch not otherwise
NO Burning and stinging |
q No erythema
q Edema reduced q On examination: No oozing no discharge HGT: 98mg/dl CBC : WBC count 10300 |
Tarentula cubensis 200,
2 hourly |

| Fig 10. Photo of the left foot after treatment |
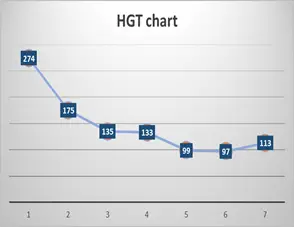
| Fig 11. Blood Sugar levels Normalised on treatment |

| Figure 12: Day 7 Complete Recovery, Photo of Left foot, No signs of infection |
References:
- Samuel Hahnemann. Organon of Medicine, 6th Edition, Indian Books & Periodicals Publishers, New Delhi, 2005, 260, IB0405
- Samuel Hahnemann., The Chronic Diseasse, Their Peculiar Nature And Their Homoeopathic Cure, Theoretical part with word index, Rearranged & augmented edition, U.P., India, 2005
- Cyrus Maxwell Boger – A Synoptic Key of the Materia Medica: A Treatise for Homeopathic Students: Rearranged & Augmented Edition: 1
- Krall, L. and Beaser, R., 1989. Joslin diabetes manual. Philadelphia: Lea & Febiger.
- Loscalzo, J., Fauci, A., Kasper, D., Hauser, S., Longo, D. and Jameson, J., n.d. Harrison’s principles of internal medicine.
- Clarke, J., 1900. A dictionary of practical materia medica. London: Homoeopathic Pub. Co.
- Boericke, W., 2005. Pocket manual of homeopathic materia medica & repertory. New Delhi, India: B. Jain.
- Phatak, S., 2005. Materia medica of homoeopathic medicines. 2nd ed. New Delhi: B. Jain.
- Dhawale, M., 1978. Symposium on Hahnemannian totality. 3rd ed. Bombay: I.C.R. – Symposium Council.