


Background:
Turner syndrome (TS) is the most common disorder of the sex chromosomes, characterised by a partial or complete monosomy of the X chromosome. The resulting karyotype is 45X, with distinct clinical features including short stature, early loss of ovarian function, congenital anomalies (mainly cardiac but also other organs), hearing and visual disturbances and neurocognitive difficulties.
Most TS affected individuals have full scale IQ but may also face social/behavioural challenges and specific intellectual disabilities 1. Median age at diagnosis is 15 years but many individuals can go through life without ever being diagnosed of the condition.
With an incidence of 1/2000 – 2500 females born, the morbidity associated with this condition is significantly more compared to the non-affected population and is mainly from autoimmunity, osteoporosis, cardiovascular diseases, digestive diseases and anaemia2.
Primary ovarian insufficiency is strongly associated with this condition, with spontaneous thelarche and menarche occurring only in 38% and 15% of the affected individuals3. Management includes growth hormone or oxandrolone for increasing height and early initiation of hormone replacement therapy for ovarian failure.
Usually, oestrogen replacement therapy is begun around 11 to 12 years of age and continued till expected menopausal age. This is deemed necessary and beneficial to induce puberty and uterine growth and to maintain a health metabolism and skeletal health. However, many studies have raised questions about the harm from such hormonal therapy4.
Hitherto, there is no study involving homeopathy in this condition in peer reviewed literature. We present a case of TS associated with severe recurrent abscesses, managed with individualised classical homeopathy.
Case report
Case presentation: A 30-year-old lady with TS sought homeopathic treatment on 10/09/2018, for recurrent skin ulcers and abscesses. The problem began six months ago and got worse after every cycle of antibiotics. Presently she had severe pain in right axilla, left mamma, sides of the abdomen and gluteal region.
There seemed to be abscesses in all these areas. In the left breast region, and the right axilla there was purulent discharge, but in other areas they were still not discharging. She was unable to walk or sit because of the pain. She described the pain as “something will explode under the skin…it is a strong cutting pain”.
On a scale of 0 to 10 she rated her pain as an 11! She also had a fever of 38oC and fluid retention in the body with scanty urination.
Laboratory Tests: Creatinine was high; high blood glucose; Sex hormones status was as 9-year-old girl. These were reported by the patient, but the actual values were unavailable to record.
Past medical history: The girl was born with the Turner’s Syndrome features along with congenital kidney disorder. She eventually underwent kidney transplantation in 2004 with her mother as the donor. She has been on immunosuppressive corticosteroids since then.
Despite these drugs, her body rejected the kidney many times and she had to be kept on very high dose of corticosteroids at such times. When she was 15 years old, she was given hormonal therapy to induce puberty and menstruation without success. As a young child she developed occasional common colds.
Family history: Father: Kidney transplantation (she is not sure but it may have been cystic fibrosis) Mother: No significant illness; Older sister: No significant illness; Grandfather: dementia, Parkinson’s disease.
Conventional diagnosis and medications: Turner syndrome, congenital disorder of kidneys, amenorrhoea, diabetes, and suppurative abscesses under the skin.
She was on corticosteroids (Pronison), diuretics, oral antidiabetic medications. In the last six months she was given antibiotics once every one or two months (for the ulcers and abscesses)
Homeopathic case taking:
When detailed investigation was made into her complete circumstantial stress and probable causative factors, the following story was revealed.
She is a yielding person, very compassionate, with nice manners. When questioned about her parents, especially her mother she became angry. She said that her anger was explosive at home but not outside.
She had low self-confidence, but she masked that with success at work. She was a stubborn person. She drove a car herself but took her grandmother everywhere she went. She was afraid of having to start dialysis and of losing her grandmother.
All her life she wanted to prove herself to others, so she tried, and studied hard but never had the courage to try and go to college. When questioned about her traumas, it was revealed that her parents rejected her even when she was born.
She was mainly brought up by her grandparents, even though she still lived with her parents. The mother had to be forced into donating the kidney by her grandmother and she held a grudge about being forced to do it. The patient was always aware of this.
She was also constantly made fun of in school because of her appearance. However, the patient was highly intelligent and artistic and excelled at multiple jobs and was doing well for herself, even acting in the village theatre.
She never had a romantic relationship. The possible causative factor was that her mother reminded her that she never wanted to give her the kidney – following which the abscesses and ulcers began.
Level of health analysis: Although being born with a chromosomal aberration can occur at any level, the associated pathologies and the ability to raise a high fever decide the level of health. Here, the case had diabetes mellitus and suppurative issues.
Her vitality seems high as the body was capable of rejecting a foreign body repeatedly despite corticosteroids. Even during the suppurative processes she was able to raise a high enough fever of 38oC. This indicates a Lower Group B. This gives us good hope for the case. As we go through the treatment, the suppurations should become lesser in frequency and intensity and if there is a possibility, her hormones should respond.
Symptoms available for prescription:
- MIND, Childish behaviour (1+)
- GENERALITES, Abscess, suppurations fever continued (2+)
- CHEST, Abscess, general mammae (3+)
- GENERALITES, Development arrested (4+)
- MIND, Ailments from anger, vexation (2+)
- MIND, Ailments from excitement, emotional, mental symptoms from (3+)
- FEMALE, Menses absent, amenorrhea (4+)
- GENERALITES, Abscesses, suppurations (1+)
- GENERALITES, Abscesses suppurations, chronic (1+)
- CHEST, Abscess General axilla (3+)
- GENERALITES, Moon agg full (4+)
- MIND want of self-confidence (4+)
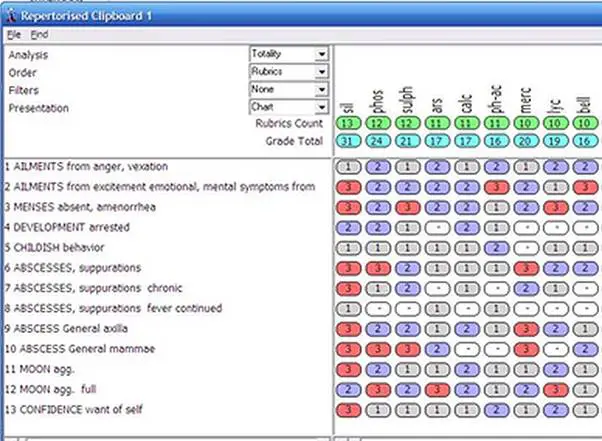
Fig. 1 Repertorisation of the first case taking on 10/09/2018
Differentiation of the remedies: Silica, Phos, Sulphur, Ars alb appeared as the foremost remedies. To the prescriber, it was clearly a Silica case. But with the background of transplantation the homeopath feared there might be a rejection and did not give her Sil.
Sulphur did not suit the case as the egotism was missing. Phosphorous required a lot more sympathetic nature and anxiety about health. Arsenicum also requires a lot more anxiety and fastidiousness which was missing in this case.
The primary pathology in this case at the moment of first consultation was suppuration and ulceration, which was also covered by Silica. However, the fear of organ rejection was strong in the prescriber.
Therefore, Myristica sebifera was chosen, based on Materia medica knowledge although it did not appear on repertorisation.
Prescription on 10/09/2018: Myristica sebifera 30C, one pill per day for one month. Patient was instructed to call every day if necessary.
Follow up:
Table 1. Follow up of the case.
| Date | Response to remedy and interpretation | Prescription |
| 15/09/2018 | 50 % of abscesses ruptured with purulent dark yellow discharge. 14 hours after the first dose. The biggest abscess ruptured and discharged dark, yellowish green, offensive pus. Temperature reduced without antipyretics. She could move her body again; she could walk and sit. Pains were much reduced | |
| 9/10/2018 | Every other day, one by one abscesses ruptured in the reverse order of their development, discharging clearer pus. Last two to rupture were under the right arm and on the left breast.
Energy was much better, creativity was better. She started to work again. Sleep was much better. Creatinine and blood sugar were still high, but better than a month ago, urination was slightly better. After the last dose of Myristica, the next day a new, small abscess appeared again on right axilla. She also developed frontal headache during the full moon and her appetite was worse. She still continued to take corticosteroids (Pronison), oral Aantidiabetics and diuretics. Analysis of the reaction: This is the is superficial action of Myristica. Urine is still scanty, with water retention in the body persisting. Creatinine and blood sugar were still high. This remedy brought about a temporary relief from pains but there was no deep action of remedy. The same repertorisation still held good (Fig.1). |
Silicea 200C one dose |
| 31/01/2019 | After the last remedy, she got high fever of over 38.5oC. She took antipyretic for the fever but that didn’t help. Multiple abscesses appeared simultaneously in the same areas as were previously affected. She suffered severe pain from these abscesses in the first week after the remedy. After this, they all began to rupture and drain bloody pus, which appeared almost black. She was also sweating profusely during this aggravation period. But at the same time, she started to urinate more frequently, 3 to 4 times in 24 hours.
Thirst become stronger and desire for meat increased. Creatinine was little above reference value but the lowest so far. After this period, she felt good, more in balance than before. Appetite became better. She has some altercation with her family, but this time was able to express her feelings. She was able to express her anger towards her mother, which she could not, before. She had some strange dreams about her ex-friends that she fought with them, and dreams about her grandmother being dead. The headache during full moon persisted and she still did not have her menses. No change in conventional medicines Analysis of the reaction: This remedy was the simillimum! Deep action of remedy was evident with no more rejection of the kidney but expression of her physical and psychological toxins. She started to express toxic emotions as anger and suppressed rage. In the aggravation she got fever over 38.5oC, which is sign that her body was fighting well. |
Nil. Wait as all the parameters are better |
| 02/09/2019 | These last 8 months patient had small abscesses a few times, lasting 2 to3 days and resolving spontaneously. Her state is good, she is in good mood most of the time.
She had high fever in July, but it lasted a very short time. She got acne on face and back. She also had mild pain in lower abdomen every month, which she connects to the full moon. Thirst was normal, craving for juice but avoided because of diabetes. She changed her primary doctor who cared for kidneys, who reduced the dose of Pronison. She suffered more from warmth than before. Urination was normal at 4 times in 24 hours. She started acting in local theatre and she got awarded as best amateur actress of the year. Her business was also doing well. She felt more confident than before. She developed cold and sore throat three times in the last four months. She didn’t use any remedies or antibiotics for these. Last month she had an inflammation of left ovary (gynaecologist diagnosis). She used herbal/traditional medicines to treat that pain. She had diarrhoea from time to time. She developed fear of dark, which she had many years earlier. All tests are normal except creatinine which is little above the reference value Analysis of the reaction: Eruptions on skin and ovary inflammation seemed to indicate puberty and activity in the ovaries!! More often colds and throat aches appear to indicate an elevation in the health level to upper Group B. there seems to be a change in the picture with her becoming more warm than chilly. Current symptoms were repertorised again (Table 2) |
Sulphur 200C one dose |
| 02/11/2019 | Patient got her menses for the first time.
Ulcers no longer appeared on the skin. Since had received kidney transplant, corticosteroids were still used. She progressed mentally and emotionally in terms of a better mood; she turned her hobby into a successful business. She got her period twice a year till date (Feb 2022). |
Table. 2. Symptoms for repertorisation on 02/09/2019
- SKIN, Eruptions, general (1+)
- FACE, Eruptions (3+)
- FACE, Eruptions, acne (4+)
- EXTREMITES, Uncover, inclination to Feet (3+)
- GENERALITES, Food and drinks, sour, acids desires (2+)
- MIND, Injustice, cannot support (4+)
- MIND, Artistic aptitude (3+)
- FEMALE, Pain General ovaries, left (1+)
- MIND, Fear of dark (1+)
Discussion:
While chromosomal anomalies cannot be changed with homeopathic remedies, the associated functional pathology may be alleviated to a great extent. In this case of Turner’s syndrome, the same may be appreciated. The patient had multiple comorbidities and all of them became better with classical
homeopathic treatment.
Initially, the homeopath was extremely apprehensive to give the remedy Silica as it is known for expulsion of foreign material from the body. On the contrary, when prescribed based on principles of individualisation, Silica helped the patient to accept the kidney and calmed her immune system down, after a period of aggravation on the more superficial level.
This phenomenon requires further investigation to investigate the role of individualised homeopathic remedies in cases of organ rejection. However, these require a high-profile hospital set up to be carried out.
What can be learnt mainly from this case for the outpatient practitioners is that even in conditions of chromosomal anomalies, classical homeopathy can offer great relief to the suffering. Another point of great learning here is that when a ‘similar’ and not a ‘simillimum’ is prescribed, one still appreciates betterment at the local level for which it is prescribed. This works as a caution because many homeopaths use the approach, where they prescribe based on partial symptomatology, without deeper investigation into the cause of the pathology and the changes in the immune profile.
Such superficial symptom-based prescription will also result in “some” effect, leading one to be misguided regarding the direction of the case. A closer inspection will reveal that the case is either where it was or may have become worse on the deeper levels.
Such practice is more akin to the conventional approach where each condition is given a separate medication. Classical homeopathy, however, can effect much deeper changes, when practiced right, and can turn a person’s life around.
Here, we see that at an age of over 30, the treatment was able to establish ovarian activity and start menses. One wonders if more could have been achieved if the treatment was begun much earlier. She was able to overcome her hatred, inhibitions and fears and achieve peace and success as the remedy freed her of these shackles.
Conclusions:
This case of Turner’s Syndrome with multiple comorbidities was benefited with individualised classical homeopathy. We need larger, hospital-based investigations to confirm the role of classical homeopathy in cases of chromosomal abnormalities and transplant organ rejection.
References
- Björlin Avdic, H., Butwicka, A., Nordenström, A. et al.Neurodevelopmental and psychiatric disorders in females with Turner syndrome: a population-based study. J Neurodevelop Disord 13, 51 (2021). https://doi.org/10.1186/s11689-021-09399-6
- Gravholt, C.H., Viuff, M.H., Brun, S. et al.Turner syndrome: mechanisms and management. Nat Rev Endocrinol 15, 601–614 (2019). https://doi.org/10.1038/s41574-019-0224-4
- Dabrowski E, Jensen R, Johnson EK, Habiby RL, Brickman WJ, Finlayson C. Turner syndrome systematic review: spontaneous thelarche and menarche stratified by karyotype. Hormone Research in Paediatrics. 2019;92(3):143-9.
- Viuff MH, Berglund A, Juul S, Andersen NH, Stochholm K, Gravholt CH. Sex hormone replacement therapy in Turner syndrome: impact on morbidity and mortality. The Journal of Clinical Endocrinology & Metabolism. 2020 Feb;105(2):468-78.


