

Introduction
In 1790, while translating a major medical text of the time, Hahnemann made himself an unusual cup of tea. Pondering the power of Cortex Peruvianis, or Peruvian Bark, in the treatment of fevers and not accepting the facile explanation that the acknowledged success using it was due to the plant being very bitter, he made a tea of this strange plant and took it himself – with unexpected and joyous results. He came upon the idea that medicine can be curative if it duplicates the symptoms existing in the patient. We all know this story and we know that this principle has guided us for the last 200 years.
Now here is the question for you? Are there any other rules for prescribing? Once we accept the idea of similarity of medicine to illness, we are still faced with the difficulty of finding this similar medicine in a consistent and accurate manner. All have grappled with this and I do not think it an exaggeration to say that finding the simillimum for the chronically ill patient is very, very difficult.
Various ideas have been, and are still, presented to the profession as the “key” to successful prescribing. In Hahnemann’s time an early one was the use of isopathy. Think how simple prescribing would be if one needed only to use the substance that caused the problem in the first place. Of course, this could be a little difficult in the case of a “hit and run” accident. Still this idea is an old one and some of you may have heard of the practice, that preceded isopathy, of treating the ax or sword that caused the wound, e.g., applying the medicine to the weapon instead of the patient. A veterinarian, Magister Lux, brought this into homeopathy as isopathic prescribing – a development that greatly vexed Hahnemann.
Another idea that has continually had appeal is to use of more than one remedy at a time – in combination (“the body will choose what it needs”) or in alternation, back and forth, back and forth between two or more remedies. Others are drawn to the use of physiological doses of medicines to treat particular organs or pathologies. Today we hear of a variety of other methods – searching the psyche for the clue, recognizing the emotional barrier one has put up because of being hurt in the past, going through the entire history of the individual and sequentially treating everything that has ever occurred, categorizing the person according to the various kingdoms of nature, and so on.
In this presentation I want go back to Hahnemann’s time with this question: Did Hahnemann ever add refinements to prescribing, beyond the idea of using the similar medicine? Well, the answer is interesting. He did add another “rule” to practice, one that is not used very much today. This is based on his discovery of the existence of the chronic diseases and what we might call “miasmatic prescribing.”
The Chronic Diseases
Considering that Hahnemann’s professional career spanned almost 50 years it is not surprising that his perspective on the basic issues of health and disease should change over that time. His greatest challenge was having a patient that he could not completely cure. Once he came to realize this as a specific problem, he struggled with it for 12 years. Imagine working alone all that time, with patient after patient and no one to guide him, trying to solve what must have seemed an impossible problem, not knowing if a solution was even possible. But he did make a discovery, one he considered the greatest of his career. This discovery was the existence and the nature of chronic disease.
The immediate problem was one we all experience. The patient would do well at first and then the disease would come back even worse than before. Then resorting again to the remedies used successfully last time, he found they would no longer work. Then would begin the cycle of remedy after remedy with increasing despair until finally the patient would either die or give up and stop treatment. Here was what Hahnemann said about such cases and we can appreciate the pathos in the statement: “Their beginning was promising, the continuation less favorable, the outcome hopeless.”[1]
I think it interesting to see the phases Hahnemann went through in relationship with this clinical challenge. We see it mirrored today with contemporary practitioners treading the same path, repeating history without knowing it. The first thing Hahnemann assumed was that there were not enough remedies, that the ones he had been using up to that time simply were not similar enough. Realize that provings of remedies were continually going on during these years and the number of remedies available was growing steadily. Hahnemann himself proved 106 remedies. So it is completely understandable that he would think it was just a question of time until the right remedies were found. But as he struggled with this problem over a period of many years, from 1816 until the publication of the Chronic Diseases in 1828, he came to realize that this was too simple an answer. He says in the Chronic Diseases that he held to this idea for a long time until he saw, as the years went by and more and more remedies were developed, that the success in chronic disease treatment was not improving. The conclusion he reluctantly came to was that it was not a lack of remedies that was the obstacle. We see this same idea coming up today – that the answer for difficult cases is the use of what are called “small remedies”, remedies off the beaten track so to speak. Hahnemann thought this too but came to a different conclusion as he studied the problem.
His next idea was that there was something different about these patients, that in contrast to what was usually seen as the more simple, straight forward prescribing for the average patient, that there was difficulty accurately matching the remedy to the patient on the basis of presented symptoms. He came to think that the illness seen was only a fragment of a much larger disease – a disease too big to manifest fully in any one person.
I don’t know how he was able to come to this but a hint is given when he used the technique he had already developed for dealing with epidemics, that is, to group patients together to assemble a fuller picture of the one disease affecting the population. Remember that he had already learned that an epidemic disease arising in a particular season would affect hundreds or thousands of people, all of whom would be suffering from the same disease at that time. They would almost all need the same remedy.
Hahnemann used this idea to study chronic diseases. He grouped patients together gradually developing a full picture of what he called psora. Can you see the similar thinking to dealing with epidemics? In contrast to the individual disturbances of a patient, each distinct from another and requiring an individualized remedy, he was using the model of treating epidemics in which all the people would need the same remedy.
One of the most interesting implications of this way of thinking about chronic disease is that treatment of psora, like the treatment of an epidemic, is suitably treated by a limited number of remedies appropriate for that condition. The difference from an epidemic, needing one remedy, is that psora has existed for a long time. It does not come and go like an epidemic does but is constantly developing itself, evolving over hundreds of years. We might say it was endemic to the human population of Hahnemann’s time. So the difference from the epidemic was that more than one remedy was possible. Still the number of remedies that were similar to the whole disease was limited.
Early on this list of remedies suitable for treatment of chronic diseases was very small. Hahnemann writes to his colleague Stapf: “You are now acquainted with the estimable remedies, you have them and can employ them, empirically at least, for you know even what doses to give them in.” “Be reasonable, therefore, and do what you can with your antipsorics. Even after I had them I did not at first know what they would do. You may, while using them, make excellent observations on their peculiar effects and gain much knowledge respecting them, as also by the many splendid cures you may perform with them, as you have only six or eight medicines to choose from, and not from the whole materia medica.”[2]
Hahnemann concluded that the reason for lack of success prior to this understanding was that these chronic cases were being treated like they were any ordinary garden variety case, using the remedy most similar to the symptoms recognized in the patient. But this did not work because the remedy had to be similar to the whole chronic miasm, not just the fragmentary part seen in that particular patient. Once he had this worked out, he began to develop a list of the remedies that were similar to the whole miasm. These he called the antipsoric medicines. Much of his exposition of this theory, his book the Chronic Diseases is a materia medica of these very remedies.
The Troubling Theory Of The Chronic Miasms
I think we can see that this was a major change from the way that homeopathy was practiced before. With the treatment of acute conditions it was a straight forward process of using the totality of observed symptoms to see the remedy needed in the case. This changed – to the idea that, in the chronic disease patient, there were only three diseases possible, each of which needed a specific group of remedies to treat them.
Hahnemann first shared his discovery with a few of his closest colleagues. His idea was to give them a foot up in the treatment of these cases. He planned to publish all of this and make it widely known, but that would take time and in the 1900’s publishing a book could take a very long time. So Hahnemann brought it to the attention of two colleagues. He thought that they would welcome it and also be able to help him to gain experience with the development of this new method.
For instance, in a letter to Stapf, he writes “I have cause to be thankful that you do not need to regard the chronic diseases as paradoxes or inexplicable phenomena, the nature of which is hidden in impenetrable obscurity. You possess now the solution of the riddle why neither Nux vomica, nor Pulsatilla, nor Ignatia, etc., will or can do good, while yet the homeopathic principle is (correct).”[3]
He goes on to encourage them to get started with the method as they will have a head start on everyone else.
“You and Gross are the only ones to whom I have revealed this matter. Just think what a start you have in advance of all the other physicians in the world. At least a year will elapse before the others get my book; they will then require more than half a year to recover from the fright and astonishment at the monstrous, unheard of thing, perhaps another half year before they believe it, at all events before they provide themselves with the medicines, and they will not be able to get them properly unless they prepare them themselves. Then it is doubtful whether they will accept the smallness of the doses, and wait the long time they ought to allow each dose to act. Hence, three years from this time must elapse before they are able to do anything useful with them.”[4]
Why did Hahnemann have to encourage Stapf so much? You would think that he would be eager to proceed with the new method. The reason for this is that both Stapf and Gross were unable to accept it. Here is the description of their reaction in Handley’s book In Search of the Later Hahnemann:
When Hahnemann first propounded the theory of the miasmatic nature of chronic disease “to his closest colleagues Dr. Stapf and D. Gross in 1827 after having worked on it in private for some 12 years , “The two men were horrified, fearing that such a wild idea would bring further contempt upon a homeopathy already scoffed at because of the smallness of its doses. They pleaded with him not to publish it. However, for Hahnemann it had now become the bedrock of this medical theory: He could not suppress an explanation of disease which seemed to him to hold out the promise of a means to cure it. He published the ideas in Chronic Diseases in 1828, and shortly afterwards began to introduce into his practice, methods of prescribing which were the consequence of the new theory. Hahnemann’s miasm theory, as it has become known, has been a difficulty for homeopathic practitioners ever since. Some have responded like Stapf and Gross, with embarrassment; others have seen it as the most brilliant contribution of homeopathy.”[5]
The majority of homeopathic practitioners at that time rejected Hahnemann’s discovery, some saying that it was the prattling of an old man, that he had gone too far finally stepping over the line into delusion. Most did not believe it and never tried it. Even today you will find the same controversy about it, the bulk of practitioners not using this method, some even denying that the chronic diseases even exist.
The problem was this: Up until Hahnemann’s presentation of these ideas, homeopathy was a sharp departure from the medical practice of the time. It rejected speculation, relying on the empirical observation of the action of each medicine as it was studied in provings. It also rejected the idea of named diseases. For example, to say that a patient had whooping cough or smallpox, some disease like that, was not quite the right way to do it. One was expected to look at each patient’s specific symptoms to find the curative remedy and to ignore whatever label was put on it by the allopaths. Here was Hahnemann now coming along and describing named diseases! I think for many it was a reversion to older thinking. In addition, it seemed too speculative, talking about the big nasty disease that could not be seen as it existed only on the dynamic level.
Listen to how Hahnemann describes these entities: “Are not the chronic miasmas disease-parasites which continue to live as long as the man seized by them is alive….”[6]. Disease parasites? Seized by them? Can we see what a departure this is from what Hahnemann had been saying before? Then, further, to make it worse, he describes psora, the grand-daddy of the chronic diseases as being contagious – spread by contact, touch, even clothing. This was different, this was strange.
This was the difficult birth of the miasm theory. So which is it? The erroneous move back into the idea of named diseases or a stroke of genius that has given us the key? Let’s look further.
Quotes From Homeopaths On Hahnemann’s Theory
Not all homeopaths rejected this. You will find Hahnemann’s ideas incorporated in the writings of many of the leaders in homeopathy, like Kent, Allen, Roberts, Close, Boericke – many names that are familiar to you.
Let’s look at a few examples of this.
We know that Kent incorporated this into his work because he wrote several chapters about the chronic miasms in his Lectures on Homeopathic Philosophy. We gain more knowledge of this as we read through his Lectures on Materia Medica in which he will give advice on the treatment of chronic cases. He refers to the distinction in cases by using the word “constitutional” to refer to miasmatic prescribing. For example in this passage during the discussion of kali carbonicum.
“All recurrent troubles, those that come periodically, or after eating certain articles, or from exposure, or with a periodicity that belongs to time – all these states are chronic; they are not acute troubles. They are simply a small portion of a chronic miasm, a side view, and all such cases must have a constitutional remedy sooner or later.”
This seems clear – that he is making a distinction in how to prescribe for chronic vs. acute problems. Here is another example of this thinking, from the same remedy discussion.
“You can, it is true, relieve violent pain at the first visit, but then you must look deeper and prevent your patient having more trouble. Otherwise, if you should give Belladonna or Colocynth or any other medicine that simply fits the colic (my emphasis), the trouble will come back again; you have not cured your patient; you have only palliated.”
You can see here that Kent is using the term “looking deeper” to mean finding the remedy that corresponds to the rest of the hidden miasm.
Another way that Kent discusses it has to do with how long the remedy will act in a case, that the remedies suitable for treatment of chronic disease will act a long time but the ones superficial to the case will have a short effect.
“…all remedies act rapidly, but not all act slowly; the longest acting may act in acute diseases, but the short acting cannot act long in chronic diseases.”
In the discussion of Sulphur, there is a very interesting angle on this. Unless we knew that Kent is thinking of psora as underlying this particular clinical condition we would not understand his advice. Here is what he says.
“Sulphur is indicated then in women who have suffered from the most dreadful agony in confinement; prolonged labor. Troublesome after-pains. Suitable also in swelling of the mammary glands. Then we have septicemic conditions, with purulent lochia or suppression of the lochia. You may go to a case in which, on the third day, there has been a chill, the lochia has been suppressed, the women has a high temperature and is covered from head to foot with sweat. As you put your hand under the covers you feel steam come up from the body so that you want to take your hand away, it is so hot. She is dazed and is sensitive over the whole abdomen.”
(As I read this, it sounds like what we would call metritis, a bacterial infection, quite serious and I would be thinking of remedies like Belladonna.)
He continues: “You know now the meaning of the suppression of the lochia; you have a puerperal fever on hand. Study closely for Sulphur (his emphasis) instead of hunting around among Aconite, Bryonia, Belladonna, Opium, etc. With these you will make a total failure in most instances, but Sulphur fits into just such a state and has cured many cases of puerperal fever.”
We can see how he implies that this is a manifestation of chronic disease, of psora. So that his experience is that when he sees this pattern in women, he has learned that it is not an acute illness and to treat it that way will lead to failure.
More clarity on this point as he continues: “If it is but a milk fever or mammary indisposition and the chill is only acute, then your short-acting remedies will do very well and even Aconite has been useful, but when it is a case of septicemia Sulphur goes to the very root of it. (my emphasis)”
Can we now understand more clearly what Kent means when he uses expressions like “a deep remedy,” “a searching remedy,” “going to the root?”
Let’s move on to J. H. Allen and quote a few passages from his book The Chronic Miasms, Psora and Pseudo-Psora.
“The fact is, we cannot select the most similar remedy possible unless we understand the phenomena of the acting and basic miasms; for the true similia is always based upon the existing miasms, whether we be conscious or unconscious of the fact.”
“The nervous phenomena may be palliated by (prescribing on superficial symptoms); but it returns, and time is lost in the experiment while the physician skilled in anti-miasmatic prescribing overlooks the foamings on the surface, and dips deeper into the case, looking for the (primary cause), and applies a remedial agent that has a deeper and closer relationship with perverted life force.”
“We must always be on the lookout for the basic miasm in these cases that are so unwilling to yield to treatment. Nature always sets up, if possible, peripheral inhibitory points of disease, pathological often, but sometimes functional. If they are interfered with locally, whether (by surgery) or not, the life force sets up another inhibitory center of reaction within the organism and nearer the deeper centers of life.” This last is within a discussion of the body responding to the presence of the miasm by producing a persistent focussed lesion as part of the defensive action.
These few examples show how Hahnemann’s ideas took root for some practitioners, indeed, for most of those that we consider worthy of study.
Having come to this point, we might ask “How did Hahnemann change in response to these discoveries?” We can expect that if he really believed this, then in his later years, his practice would reflect that. Let’s look at that next.
How Hahnemann Practiced Using The Miasm Theory
As you might expect, Hahnemann’s practice began to reflect his thoughts about the nature of chronic disease. The general trend was an emphasis on the antipsorics, especially Sulphur, and frequent use of Mercurius at certain points in the case. Rima Handley, who investigated the case records of the last years of Hahnemann’s life, 54 thick volumes, put it like this: “….such a study shows how Hahnemann altered his prescribing methods in his last years, in the light of his discoveries about both chronic disease and dynamisation. It shows the process by which he abandoned the use of the single unrepeated dry dose in favor of frequently-repeated liquid doses, and the way in which he made miasmatic prescribing a major part of his system, expanding his earlier method of prescribing solely on the basis of characteristic symptoms.”[7]
“In the later stages of his practice Hahnemann frequently prescribed Sulphur alone for long periods of time, sometimes completing whole cases without resorting to any other remedies, even when clear indications for them could be seen (my emphasis). This method seems to have been as successful in achieving cure as any more individualizing way of prescribing.”[8]
This emphasis on Sulphur logically follows from his thoughts on the importance of psora in the underpinning of chronic disease but what I want to emphasize in the above quote is the part about continuing with Sulphur even when “implications for (other remedies) could be seen”. This is a real departure in practice. Before this, one would move closely with the symptoms of the patient always seeking the most similar remedy. Now, Hahnemann is staying with what he thinks is suitable for the larger, mostly invisible, underlying miasm.
Here are some examples from his practice:
“For instance, M. Persin came in 1839, suffering from pain in the urethral canal consequent upon venereal disease. He had had more than twenty recurrences of a discharge since he had first contracted gonorrhea at the age of seventeen. Sulphur interspersed with sac lac was used for a long time in preference to apparently better indicated gonorrheal remedies, such as Thuya, which in earlier days Hahnemann had been quick to use in cases of this kind. In 1840 the sculptor David d’Angers had his arthritis controlled with Sulphur and sac lac, while in 1841 the cellist Max Boehrer was freed of cramps in the fingers of his bowing hand with this single remedy. Mme Moreau came in June 1841, suffering from the long-standing effects of smallpox vaccination and of numerous medications including mercury, as a result of which she had lost all her teeth. Hahnemann treated her uninterruptedly (and successfully) with Sulphur and sac lac for several months.”[9]
“We can see that by the time he came to Paris Hahnemann had considerably simplified his method of remedy selection. This was mainly because his ideas about the simillimum had changed a great deal since the days he intended it to cover the totality of the visible symptoms of the patient. Now, with a whole new theory of chronic disease behind him, he was determined to deal with the invisible symptoms too.”[10]
“It is in the method of choosing the remedy for the patient that these casebooks manifest some of the most important discrepancies between the received information about Hahnemann’s prescribing and the actual facts. Whatever Hahnemann might have thought and written in his early life, it is clear that in his later days he became a miasmatic prescriber. His clear intention was to treat the psoric miasm before beginning any other treatment of more individual symptoms.”[11]
What then was the place for the other remedies, the ones that were not useful against the miasms? Hahnemann writes that they are to be used when the chronic process has become acute, when it has flared up, or as intercurrent remedies for uncomfortable times or interferences like injury or grief.
According to Handley, “Despite the theoretical support for an initial prescription of Sulphur in every case, there were several situations in which Hahnemann did not begin treatment with the antipsoric. When a patient came for a first consultation in an acute phase of illness, he normally prescribed for the acute state first.”[12]
“For example, when M. Barré, the umbrella-maker, came for his first consultation the day after a major attack of epilepsy, still suffering from smaller convulsive attacks in its wake, Hahnemann treated him with Valerian every two hours for two days during the acute attacks, then with Cuprum every two hours. When these attacks had subsided he began to treat the underlying case with Sulphur, followed by a series of remedies in response to the emerging symptom picture, and finally with Sulphur again for some weeks. He succeeded in completely eliminating the problem….”
“When Mme Rougier came with lancinating pains around the heart and continuous palpitations, Hahnemann prescribed Causticum every hour in the first instance, followed by Pulsatilla and Valerian and only went on to Sulphur when this condition had improved a little. When M. Dupart came for treatment in the middle of a gonorrheal discharge, Hahnemann gave him Cannabis immediately. Only when the acute symptoms had subsided did he begin to treat the underlying case with Sulphur. When M. Voisin de Gartempe consulted him, speaking darkly of domestic vexations, perpetual anxiety, melancholy, discontent with himself and thoughts of suicide, Hahnemann gave him Staphysagria immediately and, when it did not help, went on quickly to Aurum.”[13]
This quick overview gives us, perhaps, an idea of how Hahnemann used homeopathy in his later years. It might be interesting to add what he did not do. He did not prescribe on the healthy characteristics of his patient, their likes and dislikes, preferences and so on. These expressions of individual personality were put aside in preference for the symptoms of illness. “He prescribed largely on the basis of pathological symptoms, and the patient’s physical pathology was taken fully into account and not regarded as subsidiary.”[14]
He did not give special significance to psychological symptoms. “Although in the Organon he wrote eloquently about the importance of such symptoms, he also stated clearly that this was because they tended to be more characteristic than others, not because they were psychological symptoms as such.”[15]
“In the early years of homeopathy, the years contemporary with and immediately after Hahnemann, the interpretation of materia medica tended to concentrate on physical pathology and clinical detail, exemplified in the works of Jahr, Boenninghausen, Allen, Hering, Farrington and Boericke.”[16]
“It would not be true to say that Hahnemann never prescribed on ‘mental’ symptoms. What it is important to realize is that he did so only when such symptoms were both pathological and highly characteristic of both patient and remedy.”[17]
“Hahnemann was not an essence prescriber….He prescribed only on ‘sick’ symptoms, pathological symptoms, or symptoms which, while compatible with health, were not desirable, as in ‘lachrymation while walking into the wind’ or ‘craving for the taste of charcoal’. “However neither was he a specific or a symptomatic prescriber; he was not what we might derogatorily call a pathological prescriber. He prescribed on mental, physical, general or particular symptoms of a wide variety, but only when they were prominent (my emphasis). “Symptoms such as desire to commit suicide, bloody stools, uterine hemorrhage and paralysis of single parts were all capable of being used as guiding indications to the remedies. What they had in common was that they were more or less characteristic of the patient, in that they were either a fundamental part of the patient’s disease picture, or a peculiar and individualizing aspect of the patient. And that they were also to some degree characteristic of a particular remedy. “Hahnemann was a gestalt prescriber, assuming that the foreground symptom implied the whole, that if he saw a trunk the animal was an elephant and not a tiger.”[18]
If we are to summarize the way Hahnemann practiced in his later years we could say that his medicines were directed against the underlying miasm, first of all, and that he based his miasmatic prescriptions on the changes due to the presence of disease, emphasizing characteristic mental symptoms and the physical condition of the patient and not emphasizing one over the other.
Case Examples
How can this approach be used in our cases? I will give a few examples of how I have done it. These are representative of my practice. Though some of my cases get only a remedy that Hahnemann would call an apsoric, e.g., remedies not used to treat a miasm, the ones I am presenting here all show how they end up responding to one of the remedies used to treat the miasms.
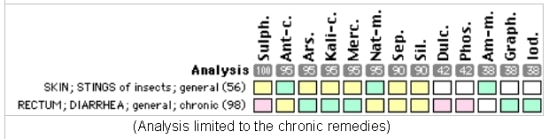
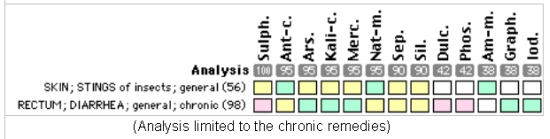
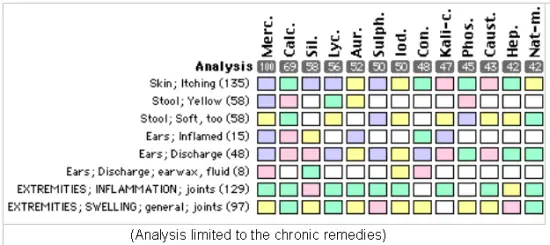
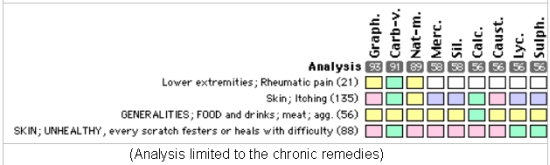
Basically, when an obvious remedy does not seem to work I then assume there is an underlying miasm and limit the remedies under consideration to the antipsorics, antisyphilitics and antisycotics. So, an analysis may indicate what seems to be a well indicated remedy, like Nux vomica for irritability, chilliness and aversion to company for example, but I will pass over that remedy for one not so similar in the analysis just because it belongs to the group of anti-miasmatic remedies. I have a filter in my computer program that limits the analysis to just those remedies suitable for the chronic case.
Where it seems to be difficult is to know if one of these remedies is appropriate at the outset or if the case should be treated with what Hahnemann called the apsoric remedies (what I call “acute” remedies for sake of a better word) instead. As we saw, he often used these remedies at first in some cases. My guide has been that if the symptoms seem to have come on quickly and are intense I use the acute remedies first but if the sickness is one with deep roots and not really different than it has been for quite some time, then I start with a chronic remedy.
Case 1
Jan. 2, 2001
Pot-bellied pig, born Dec. 2000. Was small at birth. Never nursed well. Can’t walk properly, is stilted and slow. Lies down or walks on knees or on attempting to walk in usual position, the knees knock and wobble. Either has no energy or doesn’t feel good. She acts cold, shivers, but seeks out cold corners. Client operates an animal shelter and has several other pigs. This one is the most friendly and affectionate, liking human attention.
Rx Pulsatilla 30, SID for 3 days.
Jan. 23, 2001
Not much change. Walks on knees.
Rx Calcarea carbonica 10M.
Feb. 14, 2001
Has grown to almost normal size. Improved right after remedy. Walks and runs normally.
X rays recently taken have shown that the knees and elbows are not calcified. Prognosis of permanent or long-lasting illness.
May 10, 2001
Has continued fine. Knees normal. No wobbling or knocking. Runs normally.
Still smaller body than other pigs.
August 14, 2001
Still doing well, active and moving normally.
Comments: It is interesting that Calcarea was the remedy needed in this case when the patient presented with a desire to be in the coldest corners. One would think that Pulsatilla would have had some effect, but no. It took the antipsoric remedy to move the case.
Case 2
July 17, 1990
One year old male horse with skin lesions due to insect bites. Appear as little pits that are yellow with swellings underneath. Not painful, but a little sensitive to heat. He sheds hair excessively and rubs up against things. There are many insects about and he is bitten extensively. Rubs his face from the bites and is especially affected at the outer corners of the eyes. When bitten becomes very agitated, walks in circles and swishes his tail and bucks.
Rx Ledum 200.
August 7, 1990
A little better but condition continues, patches not healed, areas scabbed and callused.
Several other remedies tried, including Apis and Thuya. Finally responded favorably to Sulphur 10M and began to heal in September 1990. Continued problems over next couple of years. For example, after castration in October 1990, developed herniation of omentum, an 18 inch piece hanging out and requiring surgery again. Vaccinated of course. Injured eye needed treatment. Developed a diarrhea that did not respond to several remedies, remedies like Calcarea (“he’s a big horse, long body, not delicate”). Some partial responses, improvement for a few weeks or months carried us to April 1992 at which point the client moved him away and contact was lost.
November 16, 1998, an interlude of 6 years.
Client back, says diarrhea has been a continued problem off and on all this time. It happens whenever he is nervous or upset and it comes on quickly. Very sensitive and particular about his food. Gentle horse, very yielding, she says “lacking self confidence”. She calls him lazy at times, says that he can become sullen about how he is treated (who can not?); “acts as if his needs are ignored”. Are they? Client sees the horse infrequently, not daily. I buy it.
Drinks normally. Weight slightly too high. Coat average. No itching.
Based on prior history and best response of insect problem to Sulphur and emphasizing the antipsorics, one dose of Sulphur 10M.
Dec. 21, 1998
Much improved, client says “a lot”. Behavior has changed for the better, takes the lead now. Client says “Better all around. I’m surprised at the improvement. Happier with himself.” Loves to run, but not so good on the lunge line, won’t listen to her. She says “he tends to be lazy”.
No treatment.
July 5, 2001
Had no further skin or diarrhea problems or health problems of any kind. Client sold him because she could not bridle him and if she tried to ride him around meal time, he would buck her off.
Excessive appetite?
Comments: An interesting case in that the initial problem of reacting to insect bites led into persistent symptoms that indicated chronic disease. Not what I expected in a case presenting with problems with bug bites.
Case 3
Feb. 3, 1987
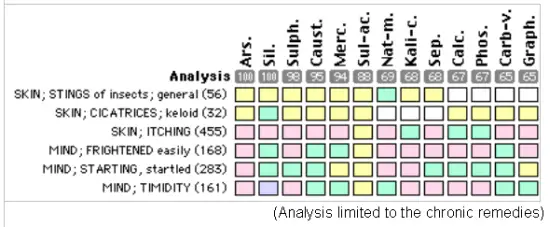
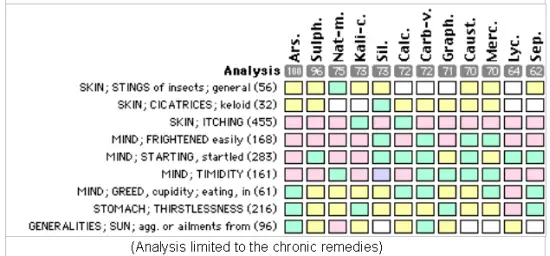
Adult horse, mother of prior case. Bothered by gnats and other insects. Rubs skin, especially the mane, until it is rubbed off, even bleeds. Skin looks grooved in affected area.
Shies easily but calms down quickly. Slightly timid. Very friendly, loves company. Seems quieter on warm days.
Treated with Sulphur 200 to 50M, single doses, ascending potencies over several months. One dose of Nux vomica 30 with coryza, cough and diarrhea during this time. Health problems resolved by October 1988.
Jan. 22, 1990
Fell in a trailer while being moved. Injured over eye and cheek. Rear left leg punctured. Pus formation. Treated with Hepar Sulph 200 orally and Calendula/saline mixture topically.
Feb. 2, 1990
Healing well. Getting proud flesh on the leg and area sensitive to Calendula applications, presumably due to sensitive condition of lesion.
Rx Silicea 200, repeated Feb. 16. Followed by Graphites 6x in March.
June 21, 1990
Proud flesh persists, low level. Itching of skin has returned. A lot of scratching of the back of ears, top of neck especially, becomes raw.
Rx Sulphur 50M – no effect.
July 17, 1990
Same.
Rx Thuya 200.
Sept. 4, 1990
Itching subsided some, not completely, and for a while. Now, very itchy, full of splinters from rubbing against wood. Same areas affected, now also the tail. No eruptions present. Client reports he now “shies at nothing”, e.g., with no apparent stimulus, therefore very nervous. Happens when riding or walking. She is frightened and timid. If taken from immediate surroundings becomes very tense and reacts to any little thing that moves. Otherwise seems healthy, a lot of energy (used to be lethargic, but no longer).
Rx Arsenicum 200.
Sept. 25, 1990
Improved with itching (as measured by amount of splinters). Behavior improved, less shying, etc. A little lethargic with change of weather to rainy.
Over the next couple of years, she needed occasional treatment for injuries, for vaccinations, for coryza. The skin itch threatened to come back once and was resolved with Arsenicum again. In 1992 a very red swollen right eye from insect bites did not respond to Euphrasia but did improve with Thuya 30 and 200. Eventually it was possible to identify exposure to cut grass and mown hay as aggravating factors. Eye became very bad again in 1992 when horse fed moldy hay. Suppressed with antibiotics and steroid.
We jump ahead, skipping an attack of mastitis resolved with Belladonna, to:
July 20, 1993
Very much more bothered by insects than usual, especially at the midline of the belly. Nothing is left of the mane – all rubbed off. Ears are bloody from rubbing. Client says “she really rubs hard.” Problem is mostly with mosquitoes and flies at this time.
Rx Caladium 10M (Hering: Fly bites itch and burn severely. Knerr: Injuries, bites, mosquitoes, burn and itch intensely) – Partial effect, not satisfactory.
October 5, 1993
Itching has moved to shoulders and neck. Rubs until bloody.
Rx Pulsatilla 10M (Hering: Itching, fine sticking sensation in skin, as from numerous fleas).
Nov. 5, 1993
Mood much better, happier and more friendly. Mane growing in. Ears are OK. Not rubbing so hard, but still some itch. She continued to improve, doing fairly well but never completely resolved until:
June 6, 1994
Rubbing out mane again. Lots of mosquitoes.
Rx Pulsatilla 10M – no effect.
June 27, 1994
No change for the better. More obnoxious. Cries at gate to be fed. Belly is big. Not much thirst. Shies easily. Demanding. Greedy. Stands in the shade rather than in the sun. Stays off by herself, even when other horses present.
Rx Arsenicum 10M. (because a remedy that was effective before, also an antipsoric.)
July 5, 2001
Remained free of symptoms from last report until sold some years later. Had no lesions or other troubles. However, client stopped vaccinating after last Rx. At time of sale, was healthy and no symptoms.
Comments: In hindsight, this looks to be an Arsenicum case all along. The behavior, when it was aggravated, would also fit this remedy. Though the problem seemed caused by severe insect assaults, still response to remedies like Caladium and Pulsatilla, that seemed likely to help, was very minimal or lacking. It was the antipsoric Arsenicum in sufficient potency that resolved the case. Stopping the practice of vaccination was also very important, I think, as it seemed to often be related to upsets in this animal over the years. When we look back at the course of treatment we can see that the acute remedies, even for what appeared to be limited problems – injuries, vaccinosis, etc. – never went as far as the constitutional, Arsenicum album.
Case 4
July 24, 2001
Cat, aged 2 years, DSH, male neuter, had no symptoms prior to development of a hematoma on one ear. There were no lesions at the ear, no discharge, nothing other than this hematoma. Cause not known. No evidence of injury. Questioning did not reveal any other signs of chronic disease. Today, vet had drained ear of blood with a syringe. No bandaging or other treatment.
Rx Arnica 30, 2 doses at 4 hours.
July 26, 2001
Ear swollen again, like before. No other symptoms.
Rx Lachesis 30, hourly for 3 doses.
July 27, 2001
Ear same. Client encouraged by me to see the ear as slightly smaller. She did not buy it.
Rx Ledum 30, SID for 3 days (will time help?).
Also vitamin E, 100 IU daily for 5 days and bioflavinoids at 15-20 mg level once a day for same period.
July 30, 2001
No better. Though maybe slightly smaller yesterday. Then today even bigger.
Rx Natrum muriaticum 30, SID for 3 days. (The assumption that an antipsoric needed.)
August 2, 2001
Looks the same, not larger. No other symptoms.
My advice: Have the ear drained again to see if the bleeding has stopped. This done August 4.
August 6, 2001, morning.
After drainage of ear, it filled again. Client doesn’t want to have to resort to surgery.
My advice: Wait longer.
August 7, 2001
On coming home evening of Aug. 6, the hematoma had gone down on its own. Today, even more flat.
My advice: Continue to wait on last Rx.
August 13, 2001
“Ear is improving each day.” No other problems.
August 22, 2001
Still OK.
Comment: Interesting that several remedies that I anticipated were perfect for this problem basically did nothing. Yet an antipsoric on little other indication than that it was in that class of remedies was effective. Why Natrum mur.? I took out Carbo veg. from consideration. Where it is helpful is usually in cases more ill than this. Phosphorus cats usually have vomiting as part of their symptomatology. Calcarea cats tend large, eat indigestibles. Natrum mur., a commonly needed remedy, left by elimination. I was lucky.
Case 5
Cat with years of recurrent urinary trouble, crystals, tenesmus and several blockages, apparently blocked again. Now in a state of frequent attempts, agitation, tenesmus without even a single drop being produced for 12 hours or more. Client dreads going into the emergency hospital again. It is after business hours of course (Do these occur at any other time?). Prior attacks unresponsive to remedies like Aconitum, Nux vomica, Pulsatilla, Cantharis, etc. History of persistent red gum line.
Rx Mercurius vivus 50M.
Two hour report: No change.
Rx Mercurius vivus CM.
Urinated within 2 hours of last Rx and continued normal urinations thereafter and for the next several months (so far).
Comment: Seeing the “trunk” of Mercurius in the gum condition, I went to the antisyphilitic remedy that would have this kind of tenesmus. Was lucky again. Cat has not had urinary trouble for several months now but case likely not finished yet.
Case 6
Adult cat found with large swelling at side of face, at cheek. A small scab, size of a millet seed palpable over lesion. Presumably scab appearing from a bite. No fever, no other symptoms, no pain. History of chronic skin allergies for years with past use of steroids to suppress symptoms. No skin disease present now. Allergy diet used to control condition.
Rx Silicea 30 (an easy case I thought – confidently predicted a spontaneous drainage within 24 hours). Apply warm compresses.
48 hours later: No change. No fever, no pain, no reduction in swelling, no discharge. Normally active, eats, as before.
Rx Sulphur 30 (lack of reaction). Continue compresses.
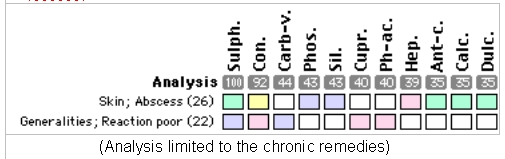
Within 48 hours, abscess opened and drained. Very offensive pus. Healed without complication. No further remedies needed. Continues well now several weeks later.
Comment: In hindsight we can see this as a suppressed case and so no surprise that it required a remedy like Sulphur to initiate an action. I don’t think any of the other abscess remedies, Myristica, Tarentula, etc. would have had any effect.
Case 7
Oct. 2, 2000
Great Dane, German import, aged 5. Vaccinated of course. Has been diagnosed with progressive retinal atrophy in the left eye by a veterinary eye specialist. Client has been noticing a slight opaque look and bluish cast to eyes for the last year. Scleras are bloodshot. Tendency to lachrymation. History of skin allergy symptoms, licks chest intensely. Doggy odor. Coat greasy. Soft stools.
Over the period of October to December, given Natrum muriaticum LM 1, Thuya 200 and Sulphur 10M. Outcome of this was basically an unchanged condition.
Dec. 14, 2000
Right eye has become cloudy. Both eyes bloodshot. No discharge but some tears from the right eye. Less chest licking. Vet exam: Sclerosis of lens of right eye.
Rx Lachesis 10M.
Jan. 9, 2001
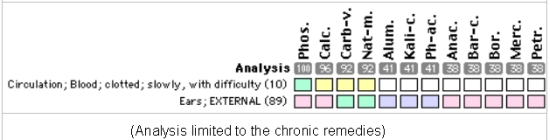
Client contacts me to say that the right eye has glaucoma, pressure 45 (normal less than 17). Hemorrhage in the eye. Dog now on prednisone drops in each eye, another drug to reduce fluid pressure, and prostaglandins.
After this treatment, at a follow-up with the vet that prescribed this treatment, the pressure in the eye was reduced to 29 but hemorrhage was so bad that eye could not be evaluated internally. Vet wants to remove the eye – suggests a possible tumor or torn lens (Figure 1). Client has discontinued drugs and asks my advice because of reluctance to have eye removed.
 Figure 1
Figure 1
Rx Lachesis 10M, given on Jan. 11. Have pressure in eye checked in 5 days.
Jan. 16, 2001
Pressure in right eye is 37. Left eye, the one with the retinal degeneration, has a pressure of 13. R. eye continues bloodshot and L. has very faint redness at the sclera.
Skin more greasy. Hair falling out more. Drinks large amounts of water “buckets at a time.”
Rx Phosphorus 10M. Report 2 days.
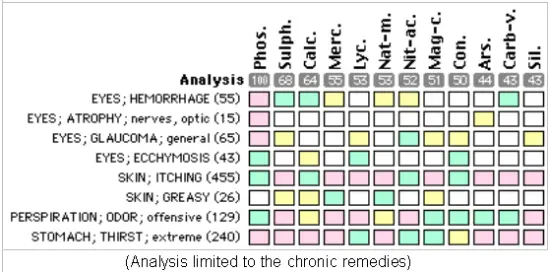
Jan. 18, 2001
Energy excellent. Less drainage from right eye. L. eye not as clouded.
Jan. 22, 2001
Fine, good energy, playful. Good appetite. Skin still greasy and hair coming out. Rt. eye pressure has fallen to 30. Vet very impressed at how well the eye looks externally.
Feb. 8, 2001
Vet: Eye looks much better internally, not bulging now. Slight clear eye discharge. Top of head feels quite hot to client.
Ultrasound of eye: “Echo dense interior chamber.” Mostly medial half of posterior chamber. Pressure now 11. Corneal diameter about 21-22 on right side; left is 17 (normal). Vet wants to remove right eye. Client does not.
Rx Lycopodium 10M
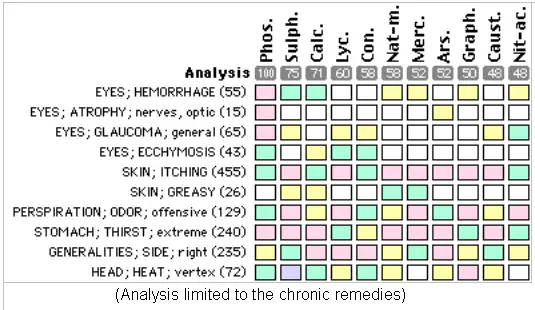
Adding in the more recent symptoms did not really change the analysis. Lycopodium decided upon after comparing the top remedies in the materia medica.
After this Rx, gradually improved in most respects. By April, the right eye had returned to normal size and shape. Client says he can see fairly well. R. eye is “marbelized red and blue.” L. eye has a greenish cast inside.
A report in June 2001 indicates that condition stable, eye smaller yet and what she considers a normal size. Still blind in that eye, has vision in left.
August 14, 2001
Still doing well. Eyes are normal size. No pain or discomfort or other eye symptoms though eye is still abnormal as to color (“marbled”). Can apparently see some as he will run into the woods and back out on the trail where he recognizes the client. It is likely very limited sight. No other symptoms, no skin disease. Feels well and is active. We discussed working further on this eye, to reduce deformity, after allowing another 2 months of stability.
Comment: I thought it especially interesting that Lachesis, a remedy I thought would control the bleeding in the eye, really had very little effect, yet one of the antipsorics used for the same indication did act well and resolved the crisis.
Case 8
This is a case of a 3 year old yellow lab, male (n.) that was obtained by the client as a puppy. Though he is not very old there have been health problems from early on. First seen by my practice in late 1999.
Oct. 28, 1999
Shy, barks. Ravenous appetite. Itching without eruptions, no lesions evident. Soft mustard colored stool. Coat thick but dull. Had been treated prior with Apis 30 to no effect. Client then gave Sulphur 30x a few times with little change.
Rx Sulphur 1M.
Dec. 6, 1999
Improved some. Sudden itch as if bitten. If eats grains will have diarrhea. Left ear irritated, likes it rubbed, scratches at it, brown discharge. Less from right ear.
Rx Bryonia 200.
Jan. 7, 2000
“Now fine. I guess the last remedy did the trick. His coat feels softer and is a little more shiny also. Eats his food like a normal dog now.” Scratching occasional and seems normal amount to client.
Aug. 14, 2000
Fractured a right premolar tooth, buccal surface. Weight now normal, very muscular.
Nothing more until May 31, 2001, a hiatus of 9 months.
Losing hair from underneath, appears to be falling out or not growing. Itchy. What hair there is too thin. Stamina not good, takes a long time to recover (dog used in rescue training). Runs well. Very painful swollen toe joint, rear left foot. Causes limping. Joint palpably enlarged. Only one joint affected. Skin darkened, odor very noticeable to me.
Abnormal lab tests:
BUN 27 (12-18), Creatinine 1.1 (.5-1.1), ALT (SGPT) 58 (3-50).
Free T4 9 (12-33), Free T3 11.6 (4.5-12), Total Thyroxine 35 (15-50), TSH 15 (0-37).
Thyroglobulin autoantibody 511 (<200).
Rx Mercurius vivus 30, SID X 3 days. Also supported with Immuplex and Antronex. On excellent diet.
June 8, 2001
Joint has swollen 3 times more than it was. T. 101.8 and rose to 102 later. Foot very tender but he walks OK. Client soaking affected foot in cold water every 15 minutes to reduce inflammation and is concerned about an infection.
Sig. Stop cold water soaks, delays healing. Toe has arthritis and will improve with more time. Report again in another week.
June 10
Began to improve. Two front paws and rear right foot developed a blister-like eruption with a reddish fluid discharge. Client opened them and applied calendula cream. Joint swelling much reduced and no sensitivity there now. Very energetic, more. Itching comes and goes, not constant. Appears to be having some new hair growth. Temperature now normal, ranging from 101 to 101.4. Doggy odor less. Stools normal, no diarrhea. Improved stamina.
An allergy testing that was recently done show sensitivity to 30 things and several borderline other substances.
July 10
“Doing wonderfully.” Has gradually improved. No limping or soreness. Hair growing back except on the legs. Hair softer, odor reduced by half. A lot of energy. Weight perfect.
July 23
Occasional itch. Still improved, stamina better, skin and coat improved.
Rx Sulphur 6c, SID X 10 days.
Aug. 6
Client notices his dog itches more when fed chicken or beef; > feeding lamb (there were not dietary restrictions based on allergy tests – advised to avoid any foods that obviously aggravated). Recently lame on right rear leg after exertion. Has had some coming and going of sores and itching and they resolve slowly.
Rx Natrum muriaticum 6c, SID X 7 days.
Aug. 20, 2001
No trouble. Went on a search and rescue certification and did very well. In great shape, no limping, no itching. Coat gradually improving.
Sig. No remedy for now. Report again.
Comment: This is a case that I considered was likely inherited chronic disease. Treating primarily with antipsorics and antisyphilitics has brought this dog into a state of health better than he has ever had before in his short life. Though not a finished case, it shows the usefulness of miasmatic prescribing as a method.
In Conclusion
In this presentation we have considered this question: Did Hahnemann use additional means to decide what medicine to use beyond the requirement for similarity between that medicine and the patient’s illness? We found that he set chronic disease into a different category from other types of illness and that he also decided the approach to these cases indeed needed a different strategy. An important part of this strategy was an emphasis on a relatively small group of remedies that he found were similar to the deeper, non-visible part of the chronic diseases he called miasms.
My experience seems to confirm this. Almost without exception my chronic cases end up on one of these antipsoric remedies. Before I understood Hahnemann’s writings about this I often found myself frustrated with the use of what seemed to be very well chosen remedies that did not have any effect in my case. After changing my approach, in the way that we have discussed here, my results improved greatly. So, I will confirm that Hahnemann’s advice seems good.
Is this idea of miasmatic prescribing a rule that does not allow exceptions? I don’t think so. I have cases that do respond to remedies in the apsoric class and they can have the same initial presentation of what I expect to see with chronic disease, e.g., I think they are chronic cases from the beginning. Is this then an exception? My thought is that these cases will need the deeper remedy later – maybe not right away but at some point when symptoms of ill health appear again. Some of these cases I do see again and can confirm this. Others I do not see for long periods or never see again and they presumably remain well, so I don’t think we can say this is an absolute rule – at least in the way that I feel that the requirement for the similar remedy is an absolute rule. Nonetheless, I think this approach that Hahnemann developed is a very useful tool and I encourage you to consider it and to try it in your own practice.
Footnotes
1 The Chronic Diseases, p. 20.
2 Bradford, p. 182.
3 Bradford, p. 182.
4 Ibid.
5 Handley, p. 36.
6 Chronic Diseases, p. 46.
7 Handley, p. 13.
8 Handley, p. 45.
9 Ibid.
10 Handley, p. 46.
11 Ibid.
12 Handley, p. 45.
13 Handley, p. 45.
14 Ibid, p. 71.
15 Ibid.
16 Handley, pp. 71-72.
17 Ibid, p. 72.
18 Ibid, p. 73.
Bibliography
In Search of the Later Hahnemann by Rima Handley, published by Beaconsfield Publishers Ltd, UK in 1997.
Lectures on Homeopathic Materia Medica by James Tyler Kent, MD, fourth edition, published by Boericke and Tafel, 1932.
Lectures on Homeopathic Philosophy by James Tyler Kent, MD published by North Atlantic Books in 1979.
Life and Letters of Hahnemann by Thomas Lindsley Bradford, MD published about 1895, p. 182.
The Chronic Diseases: Their Peculiar Nature and Their Homeopathic Cure by Samuel Hahnemann, Volume 1, Second enlarged German edition of 1835.
The Chronic Miasms: Psora and Pseudo-psora by J. Henry Allen, MD published by B. Jain Publishers Pvt. Ltd., reprint 1986.


Homeopathy eventually developed into a healing belief system. Infections were the only known diseases at Hahnemann’s time. Today we have hypertension, diabetes, cancer, etc. There is not a dongle study that merits homeopathy to successfully cure any of these diseases. What would Hahnemann do if he was alive today. Praise his on miasma theory or try to heal the sick?
What is the program or filter you use to leave you with so called antipsorics for chronic cases
I use MacRepertory program and I created a family that contains the antipsoric remedies listed in Hahnemann’s Chronic Diseases, plus a few from Boenninghausen that he also identified as antipsoric, then I added in Mercurius to represent Syphilis and Thuya for Sycosis.
Then I made a custom analysis and graph so I can toggle back and forth between all remedies and just those suitable for chronic disease.
Kent Homeopathic has put all of this into their program so you can choose my settings to run if you wish.
I loved your article. I have a beautiful Burmese cat who only has Homoeopathic treatment and, so far, has been very well. No vaccinations.