

Presented to the Second Annual Session of the Homeopathic Academy of Naturopathic Physicians, Portland, Oregon, April 25-26, 1987. (Since 1987 Dr. André Saine has seen over two hundred patients with multiple sclerosis. The results have remained the same as the ones reported in this paper.)
Introduction
I would like to address three points regarding the homeopathic treatment of the multiple sclerosis (MS) patient: Results, prognosis and case management. Before discussing these three points, I will briefly review the pathophysiology, etiology, symptomatology and natural course of MS to better appreciate the limitations, difficulties and evaluation of the homeopathic treatment.
I—Pathology of Multiple Sclerosis
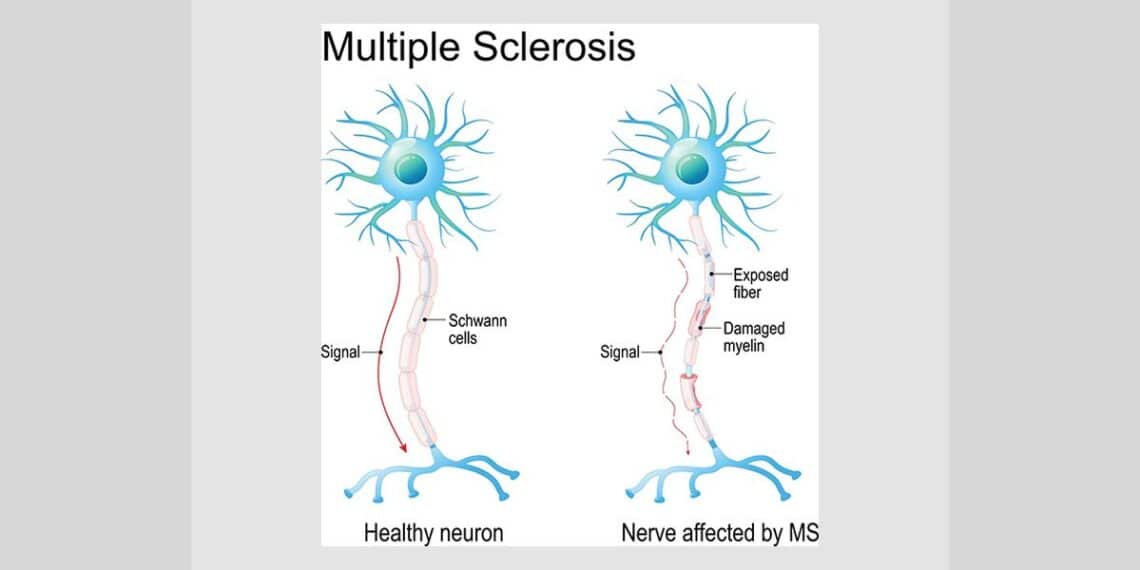
PathophysiologyMS is essentially an inflammatory disease of the central nervous system (CNS) that develops in a genetically susceptible host. Due to an alteration of the blood brain barrier (1) (BBB) and local blood circulation, (2-3) an inflammation develops along the capillaries in the CNS and destroys the myelin covering of the nerve fibers. As destruction of the myelin progresses, conduction along the axon diminishes. When this inflammation remits, the myelin returns, even in areas of total demyelination. Scar tissue (gliotic scar) may also develop in areas with severe destruction.
This process of demyelination usually starts in adolescence, but the first symptoms may not be experienced until the early to mid-twenties. They become more pronounced in the late twenties to early thirties—this is when the diagnosis is usually made. So the affected person is asymptomatic for years, in spite of the development of lesions, because nerve conduction can still occur in spite of large areas of demyelination. (4) Studies with NMR (Nuclear Magnetic Resonance) have permitted researchers to observe the appearance of lesions days before the appearance of symptoms during a period of exacerbation, and the disappearance of these fresh plaques during the period of remission that follows. (5)
Etiology
As for the etiology of MS, the literature is extensive, contradictory and controversial, but the vast majority of investigators agree that the development of MS is multifactorial and requires three factors: first, a genetically susceptible host; second, an environmentally acquired factor; and third, various stresses that act as triggering factors. (4, 6)
MS is not directly inherited but a first degree relative has 15-20 times the expected rate of occurrence. (7) Individuals of various HLA haplotypes have been identified as having a greater susceptibility to MS. For instance, persons with Dw2 and Dr2 haplotypes have more than twice the possibility of developing MS than the general population. (8-9) In a population of north-east Scotland, with one of the highest incidence rates of MS in the world, 80% of the MS patients share the same genetic marker, DQw1. (10)
The risk of developing MS is greater in people that have lived the first 15 years of their lives between the 40th and 60th degree of latitude of either hemisphere. The risk remains permanent even if the individual migrates to a more northern or southern area after the age of 15. So it appears that between the ages of 5-15 an environmental factor which affects the BBB, probably an infectious agent, is acquired while living in these geographic areas. Viruses have been the most suspected infectious agent. Most considered are measles, rubella, herpes simplex type 2, Epstein-Barr and influenza viruses. (4, 11, 12) So far, no convincing evidence has been able to strongly substantiate a single viral agent as a causative factor of MS. It is probable, however, that MS patients are more susceptible to the accumulated effects of viral infections.
Rickettsial and para rickettsial (chlamydial) infections are more probable as an etiology of MS. In 1960, Legac demonstrated to the Paris Academy of Sciences a rickettsial etiology of MS. (13) Greisman had previously reported that rickettsial toxins are angiotropic and produce severe vasoconstriction of the precapillaries and large and small arterioles. (14) Legac speculated that vasculitis of the cerebral vessels produced from latent rickettsiosis would lead to anoxia and destruction of the proximate neural tissue. In 1962, Jadin substantiated Legac’s work as he found the presence of rickettsial antibodies in the serum of 70% of 374 MS patients. (15) In 1970, Field was unable to substantiate the finding of Legac and Jadin, that rickettsial antibodies were present in the serum of many MS patients. (16) Legac severely criticized the methodology used by Field as the reactivation of all the sero-negative diagnoses was not performed as recommended. Legac had found that reactivation changes negative results into positive ones in about 60% of cases. Legac stated that “the fact of not performing this reactivation led to wrong results and also shows that the authors were undertaking research in a field which was foreign to them.” (17) The hypothesis that rickettsial infection may be involved in the pathogenesis of MS was again raised in 1980 as Szekeres found that the serum of 42 of 56 MS patients contained rickettsial-specific antibodies as compared to only 8 of 42 age and sex-matched controls. (18) The two most convincing pieces of evidence for rickettsia and para rickettsia as an etiology of MS are that Legac was able to produce rickettsiosis in laboratory animals by injecting them with the serum of MS patients, and that MS patients responded very favorably to anti-rickettsial therapy. (19)
Many different stresses have been identified as precipitating, in various individuals, the onset or exacerbations of MS. Emotional stress or trauma is of the highest importance such as grief, anger or even worse suppressed anger, rejection, humiliation, disappointment in love or business, etc. (20) Physical trauma is next in importance. 10-15% of patients experienced the first appearance of symptoms after physical injury and 50% of patients experience a relapse after physical trauma, especially concussion to the brain or spinal cord. When the brain or spinal cord of an MS-susceptible person is injured, the area of injury becomes a potential nidus for a new lesion, if the injury involves an area in or near a plaque. The latter may be reactivated and/or enlarged and become symptomatic. Cervical spondylosis and other mechanical stresses will increase the susceptibility of local spinal cord lesions. Other physical traumas that have specifically been observed to aggravate the MS patient are electric shock, (21) spinal anesthesia (22) and surgery. (23-24) Physical exhaustion, as from overworking, and lack of sleep will aggravate the majority of MS patients.
Exposure to chemicals, drugs and allergens can trigger exacerbations. Mercury amalgams, dental work and surgery, such as the removal of wisdom teeth, have also been experienced as aggravating MS. (25) Metabolic and endocrine changes related to ovulation, menstruation or following pregnancy have all been found to increase the risk of exacerbation. (26-27)
Factors known to alter the BBB, such as rickettsial and viral infection, and vaccination, have been reported to precipitate MS. Although MS patients develop 20-50% fewer viral infections (such as colds and flus) compared to the general population, they experience 3 times as much exacerbation during the months of high incidence of such infections. (28) Twenty-seven per cent of all exacerbations are related to minor respiratory tract infections. MS patients experience 4 times more sinusitis at which time their rate of exacerbation is doubled. (29)
A high incidence of MS has been reported in relation to measles, rubella, varicella and canine distemper virus. Many investigators have reported the onset of MS following vaccination. (30-31) Also, it is interesting to note that in classic post-vaccinal encephalomyelitis, 20% of patients have lesions indistinguishable from MS.
Hyperthermia, including fever, will commonly exacerbate the MS patient by inactivating the sodium pump and decreasing the action potential. So the patient experiences an increase in symptoms without a true aggravation of the pathology. Other climatic factors such as humidity, changes in atmospheric pressure or temperature can increase the symptomatology of the MS patient.
Symptomatology
The presence of symptoms depends on the frequency, severity and site of lesions or their cumulative effect on the nervous system. Each individual will present with their own set of symptoms. Common signs and symptoms of MS will include weakness, heaviness, incoordination, intention tremors, spasms, ascending paresthesia or paralysis, hyperreflexia, clonus, Babinski response, nystagmus, diplopia, visual loss, altered speech, constipation, incontinence, impotence, etc. On the mental level it is not unusual to observe euphoria, denial of illness and even schizophrenia.
Natural course
The course of MS is unpredictable. In one patient the disease may be completely benign with one or two exacerbations followed by complete remission lasting for many years, and in another, it may take a relentlessly progressive course leading to serious disability within a few months or years from the onset. A benign course may also later evolve into a progressive one in which remission does not occur.
Although the course varies from one individual to another, two general patterns exist, namely: 1) exacerbating-remitting and 2) progressive. The exacerbating-remitting course is characterized by episodes of relatively sudden deterioration followed by remission, with complete or nearly complete alleviation of the symptoms. In the progressive course, although there may be periods of relative stability, the overall course is downhill without any significant remission. (32)
After the onset of MS, there is usually less and less improvement with subsequent episodes as lesions accumulate in the nervous system. Over 70% of patients will eventually enter into the progressive phase of the illness. (33) It is important to note that less than 5% of all affected patients will go into permanent remission and this usually occurs in the first year of the appearance of symptoms. Thus permanent spontaneous remission is unlikely to happen after the first year of onset or in patients experiencing chronic episodes.
II—Homeopathic Treatment
A-Results
Discussing cases with experienced homeopaths, I find a consensus that the great majority of patients diagnosed with MS respond well to homeopathic treatment. Such cases have been reported throughout the homeopathic literature as far back as 1862, shortly after MS was recognized as a precise syndrome. (34)
In 1925, Rorke, a British homeopath and physician to the Royal family reported that seven cases treated for an MS condition, three had complete recovery, three were much improved and there was little or no change in one case. (35)
In the last two years over twenty cases diagnosed with MS have come under my care. It is difficult to precisely quantify and qualify the results obtained for a whole group without reviewing each case individually. However, attempting to give a broad summation I can report 50% excellent to very good results, 35% good to fair, and 15% poor to no results.
From these figures, I have excluded six patients of the twenty originally seen as I was unable to personally follow them up. Three of these had been referred by other homeopaths only for the first consultation.
By “excellent to very good results” are meant cases which demonstrated under pure homeopathic treatment dramatic changes in signs, symptoms and the course of their conditions, and in which there were unexpected uphill recoveries with rare exacerbations, mild if any. These include some early cases and advanced cases, but mostly chronic cases in the exacerbation-remission phase.
In the “good to fair results” group, the changes are less dramatic but nonetheless remarkable, and exacerbations decrease in frequency, intensity and duration, but can still produce severe drawbacks. More patience and care must be paid by both the physician and the patient in such cases.
In the “poor to no results” group are cases generally in the advanced progressive state, often bedridden, with almost total paralysis, or cases presenting defective illness. In some cases of this last group remarkable psychological and functional improvement are noted but with little or no improvement of the physical disability.
These results are consistent with results reported by other homeopaths. (35-37)
B-Prognosis
Because the inflammatory process of MS is reversible, as seen above, theoretically we can expect to stop the disease process in every case by neutralizing the predisposing and precipitating factors.
The extent of recovery will depend on the capacity of the organism to repair areas of demyelination and possibly also areas with gliotic scaring.
Clinically and practically speaking, the prognosis will depend on several factors which are learned through experience. I have observed the following factors as an aid to determine the prognosis:
The clarity of the case
The clearer the homeopathic case, the better the prognosis. When the totality of symptoms of both the disease and the patient correspond to one remedy, the simillimum, the prognosis is excellent. The prognosis is usually less good when the guiding symptoms lead to a remedy, the simile, that covers only a certain aspect of the case. The prognosis is very poor in defective illnesses.
The symptomatology
The prognosis is better in the presence of clear and intense rare, peculiar and characteristic symptoms. Also, if the patient is very emotional, or there is a strong psychosomatic component in the onset or exacerbation of the disease, the prognosis is good. The prognosis is very good if the symptomatology is fluctuating because of the hypersensitivity of the patient to weather, climate, heat or cold, allergens, menstruation or other hormonal influences, etc. Similarly the prognosis is very good if there are present strong associated syndromes such as hypoglycemia, PMS, problems of circulation, sleep, appetite, moods and energy fluctuations, etc. On the other hand if there is a tendency to recurrent infections, such as flu, cold, sinusitis or urinary tract infections, the prognosis diminishes if these episodes are not controlled at once.
Lastly, when the patient presents with eye symptoms and problems of vision, the prognosis is very good. With advanced cases of ascending paresthesia and paralysis the prognosis is poor. This may be partly explained by assuming that the longer the nerve pathway affected the more extensive is the damage and the less reversible it is.
The severity of the damage
The more extensive the organic change, the poorer the prognosis. If a symptom has been present without any improvement for a prolonged period (two years or more) it is usually irreversible. A recent onset favors a better prognosis.
The course of the disease
The more benign the course, the better the prognosis. Also, the remitting-exacerbating course favors a better prognosis. When the patient has reached the progressive state the prognosis is less favorable.
The patient
1. Response to the indicated remedy: The better the first response to the first prescription, the better the prognosis for the rest of treatment. The prognosis is very unfavorable when the patient responds little or not at all to the simillimum. It is not unusual to have a patient responding very well to the remedy for six to nine months, then reaching a plateau and little response follows. When the case stalls in such a way little progress can be expected for months afterwards.
2. Level of vitality: The more vital the patient the better is the response. Usually, the younger patient, the greater is the vitality and the better the prognosis. A state of sudden exhaustion does not influence the outcome but a state of chronic depression makes the prognosis unfavorable.
3. Lifestyle: The better the patient’s lifestyle, or the greater the ability to adopt a healthy lifestyle, and subsequently the adoption of such lifestyle the better the prognosis.
4. Compliance: The better the patient’s compliance with the treatment plan and lifestyle changes, the better the prognosis. On the other hand the prognosis is less favorable when the patient lives at great distance, or has poor understanding or is doubtful of the treatment plan.
Seasons and climate
The prognosis is usually more favorable when the treatment is administered between April and October and less favorable from November to March. Dry weather conditions will improve the prognosis, while cold wet weather and rapid change from warm to cold and vice versa during the winter months will greatly enhance the possibility of acute infections and ipso facto the occurrence of exacerbations.
The physician
The skill of the physician in applying appropriate homeopathic treatment is a crucial factor for the long term recovery of the patient. This is especially true regarding the ability of the physician to rapidly manage the patient during a period of crisis. The greater the experience of the physician in managing homeopathically and hygienically the MS patient the better the prognosis. It has been my experience that one of the greatest limitations of young homeopathic practitioners in prescribing for the MS patient is to limit consideration to a few remedies, such as Phosphorus, Causticum, Alumina or Argentum nitricum, claimed by many physicians to be the “best for MS.” Rorke claims that homeopaths have no specifics, “If asked what drugs they used in disseminated sclerosis, they could only put forward a list of three or four hundred and say that it might be one of those.” (35)
C—Case Management
Kent compared the learning of homeopathy to going to grade school. There is first grade, second grade and so on. We could say that first grade is to find the simillimum in a clear case. To follow a patient over several years and be able to successfully prescribe the indicated remedy in the correct potency and repetition and to understand the reaction to each remedy is for the student in the higher grades. Eight points are here presented on how to manage the MS patient over the long term.
1-A thorough case history
A thorough case history is the first requirement in developing the basic understanding needed to guide even the most difficult patient to recovery. The most traumatic events in the MS patient’s life are usually important keys, especially the ones immediately preceding the time of onset and of exacerbations of the symptoms. Past medical history can also be very important, especially regarding occurrences and reactions to infectious such as colds, flus, urinary tract infections, etc. History of bad reactions to drugs or vaccinations can be the necessary key leading to the indicated remedy, as seen in a case reported by Tyler: “Disseminated sclerosis in a boy of 19. Ill seven months: treated in several hospitals without any improvement.”
“Past History included measles, chickenpox, so bad that the doctor thought it was smallpox. Vaccinated in 1935, took very badly. This illness supposed to have been result of encephalitis.”
“First seen October 31st, 1940. Complaint, hands and head shake. One found marked tremor of hands and head. Scanning speech. Eyes affected. Variolinum 200.”
“In a month, Walks better: feels stronger. Thuja 200.”
“In another month, Thuja 10m.”
“January 1941. Head does not wobble now. Doing A.R.P. work. Can walk long distances now without fatigue. Not worried when guns start now. Thuja cm.”
“February. Still pallor in temporal half of left retina.”
“May. M.B. every way. Does A.R.P. work, and also his own electrical business. Looks well: speaks better: slight tremor of hands still.”
“June, July. Much better. Walks all right now. Has joined a Dramatic Society. Vision perfect; doesn’t even need glasses for reading. Says, ‘he has been to hospitals, etc., but no one ever helped him before.”
“September. Everything better: yet, he got a repetition of Thuja cm. and (?) not needing it, was not so good in November. Aurum 12, 3 doses.”
“December 1941. Wants another medical examination for military service. No tremor. Eyes normal. Can touch tip of nose with finger. . . . Apparently cured.” (38)
Recurrent illnesses and associated syndromes such as migraines, hypoglycemia, dysmenorrhea, PMS, etc, must be carefully noted as they often provide important leaders.
Examination of the patient
The rubrics obtained by strictly observing the patient, such as frowning, answers, reflects long, laughing over serious matters, weeping when telling her symptoms, etc, provide often more than half of the guiding symptoms in a case. Over and above this, a good physical and neurological exam of the MS patient will provide many objective signs that are extremely helpful in evaluating the response of the patient to the treatment and in important prognostic clues. The most important tests are examination of the deep tendon reflexes, the plantar reflex, the presence of clonus and nystagmus, the gait (especially when challenged by having the patient to walk heel-to-toe or on the heels, etc), the sensations, especially the sense of vibration and finally the fundus of the eyes.
Case analysis
What are the most important symptoms on which we should base our prescription? The answer is simple. It is as old as Hahnemann. In paragraph 258 of the Organon we read: “the only medicinal disease agent meriting attention and preference in any case of disease is always the one that is most similar to the totality of the characteristic symptoms and no petty bias should interfere with this serious choice.” (39) But which symptoms presented by each MS patient will be the most characteristic? To properly distinguish the characteristic symptoms from the common symptoms in the MS patient the homeopath must first have a good knowledge of pathology. Second he must complement this knowledge with learning from clinical experience in the homeopathic treatment of such MS cases as described below.
1. Symptoms that are leaders in certain remedies but are common symptoms of MS are not helpful to find the simillimum, i.e., ascending paresthesia and paralysis as in Arsenicum, Conium, Kali-c., Phosphorus, Plb, etc, or the intention tremors of Mercurius, Plb., Silicea, etc., or the hyperreflexia of Cicuta, Lath., Nux-v., etc.
2. Common symptoms of the disease that have proved to be guides to the remedy are numbness of the face, nose and tongue, especially when unilateral—these were pointed out by Lippe over a century ago as a leader for Natrum muriaticum. The great majority of MS patients are aggravated by heat. The most aggravating type of heat becomes characteristic, such as aggravation from heat in the Spring (Lachesis), or in the sun (Lachesis, Nat-c., Natrum mur.), or from a warm room (Lycopodium, Pulsatilla, Sulphur), or from a change from cold to warm weather or from warm wet weather. Burning sensations are found commonly in the MS patient, but the location is characteristic of certain remedies, such as the burning spots on the skin of Sulphur (if wandering: Pulsatilla) and burning heat of the feet, with uncovering, remains a great leader. Apparently common symptoms of the eyes have served as important guides, such as the black floaters of Natrum mur. and Phosphorus, the paralysis of the internal recti of Natrum mur. and of the external recti of Causticum and Sulph., the hemiopia of Natrum mur., Sepia and Sulph., and finally the loss of vision during menses (or before) of Pulsatilla and Sepia The rubrics under Side in Generalities have been found helpful to confirm a remedy, such as crosswise, left upper and right lower (Natrum mur., Pulsatilla, Sulphur), or right upper and left lower (Causticum, Lycopodium, Phosphorus), right to left (Causticum, Lycopodium, Phosphorus, Sulphur) and left to right (Lachesis). Great aggravation from lack of sleep has often pointed to Causticum, Nux-v. and Sulph.
3. Lastly we have the true characteristic symptoms of the disease. These rare, unusual and peculiar symptoms which are the result of the patient’s idiosyncrasies have been found to be the most important leaders for prescribing. It is very peculiar to have all the symptomatology of the MS patient aggravated when hungry (Lycopodium, Phosphorus, Silicea, Sulphur), before the menses (Lachesis, Pulsatilla, Sepia), before a storm (Phosphorus, Psorinum, Rhododendron), at 10-11 AM (Natrum mur., Sepia, Sulphur), at 4 PM (Alumina, Causticum, Lycopodium), in the evening at twilight (Phosphorus, Pulsatilla), by windy weather (Chamomilla, Lycopodium, Nux-v., Phosphorus, Pulsatilla, Rhododendron), by dry weather (Causticum), by cold wet weather (Medorrhinum, Rhododendron, Rhus-t.) or by tight clothing (Lachesis, Sepia).
4—Education of the patient
Education is the first duty of the physician. At the time of the first visit the patient must not only be educated on homeopathy and its possibilities but must also be provided with all the necessary instructions for proper homeopathic treatment. Care must be taken that the patient knows to immediately contact the physician at the first sign of a relapse or at the beginning of an infection, especially during the winter months. Next the patient must be advised to adopt a lifestyle that is conducive to good health. This aspect of treatment may be the most important for enhancing the patient’s long-term recovery, but is the most difficult for the patient to achieve. First the patient must get sufficient rest and sleep. It is crucial for the MS patient not to get depleted by overstimulation, overworking, over exercise, or missing sleep—as from partying, for example. Rest must be balanced with adequate amounts of exercise. Russell, a professor emeritus of clinical neurology at Oxford, has observed that athletes in full training were virtually protected from developing MS but become more vulnerable two or three years after abandoning their training. In the early 1960’s he developed a rest-exercise program (REP). He followed 69 patients for 15 years or more and found that there was no relapse or exacerbation as long as the REP was well conducted. The patients were able to virtually arrest MS just by adopting a disciplined program of rest and exercise. The REP of Professor Russell consists essentially of 2-3 periods a day of 5-10 minutes of building up to quite violent aerobic exercise, followed by a period of lying down in complete relaxation for 10-20 minutes. (40)
Good diet will also play an important role in the long-term recovery of the MS patient. The patient must avoid all foods he is intolerant of and abstain as much as possible from processed foods, especially sugars, grain flour and alcohol, and stimulating foods such as tea and coffee. The patient should adopt a diet which is individualized to his needs. A diet low in animal products and high in raw unprocessed vegetables, fruits, nuts and seeds is preferable in many cases. Such a diet is supported by findings of scientific studies investigating diet and dietary supplementation in the MS patient. Swank found that 95% of patients diagnosed with MS and with minimum neurological involvement suffered no further disability if in the first year of appearance of symptoms they adopted a diet low in animal fat. (41) Other researchers have found that a diet high in certain fatty acids will reduce the severity and duration of exacerbations without affecting their frequency. In the assessment of three double blind trials, a diet rich in linoleic acid (such as found in sunflower seeds) was found superior to both placebo and to a diet rich in oleic acid (as found in olives) for decreasing the severity and duration of exacerbations. The patients with minimal disability at the entry did not have significant change over the course of the trials, whereas control patients had a significant increase in disability. (42) Diet rich in eicosapentaenoic acid (EPA) as found in cold water fish has also been found to reduce the intensity and duration of exacerbations. (43) Sinclair had observed that the occurrence of MS in Eskimos was extremely rare in spite of a diet rich in fat. (44) But he postulated that a diet high in EPA would decrease the platelets stickiness and capillary fragility as found in MS patients. (45-46)
Increased peroxidation has been suggested as a pathological process in MS. (47) In agreement with that a decreased glutathione peroxidase activity and linoleic acid content in hematogenous cells from MS patients has been documented. (48-50) Supplementation with antioxidants (6.6 mg. of sodium selenite, 2 gm of vitamin C and 500 I.U. of vitamin E per day) increased and normalized within 3 weeks the glutathione peroxidase activity and the cellular content of linoleic acid. (51)
In an uncontrolled study patients showed a decrease of more than half the number of exacerbations when taking supplementation with calcium, magnesium and vitamin D. (52) Magnesium glutamate supplementation has been used for many years with great restorative effects in the treatment of MS patients by my father, Dr. Joseph Saine, in Montreal.
It is important that the MS patient avoid contact with toxic chemicals and fumes and choose an environment as free from pollution as possible. Many patients have reported the onset or exacerbation of symptoms after exposure to these agents.
Regarding the removal of mercury amalgams from the teeth, great care must be taken. Homeopaths have reported toxicity from these amalgams since their first use around 1840.53 H.C. Allen used to have his patients removed their amalgam fillings almost systematically. (54) In my experience, some MS patients have experienced great relief while others have suffered severe drawbacks from removing the amalgams. The sudden removal of these amalgams at the time the patient’s resistance is low can precipitate a severe exacerbation. I recommend the more vulnerable patients have their amalgams removed at a time of greater resistance by a competent dentist using all possible precautions to minimize trauma and further intoxication. Each dental session should be kept to less than 90 minutes and at only one tooth should be worked on to better evaluate the strain caused by the removal.
5—Supportive approaches
1. Stress reduction is crucial. This can achieved through inner changes and through changing of one’s lifestyle. Priorities should be established and goals should be set. The patient is encouraged to live a life which is more in harmony with their needs. Exercise including yoga, arts such as music, painting or dancing and meditation are encouraged.
2. Hydrotherapy in the hands of the trained physician is an ideal treatment to enhance the oxygenation and circulation of blood, to increase the oxidation and elimination of toxins, and to assist in the restoration of nervous equilibrium. Alternating applications to the spine and cold friction rubs would well complement constitutional treatment for both the acute and the chronic states of MS.
3. Electrotherapy has also proved to be very useful in stabilizing the MS patient. Bioccular transcerebral iontophoresis has shown remarkable results in most patients with MS in decreasing the accumulated scar tissue in the CNS and restoring normal nervous equilibrium. Ultra-violet and infra-red light can be applied daily especially during the winter months. The infra-red light seems more beneficial when applied to the palms of the hands and the soles of the feet 5-20 minutes daily.
4. Acupuncture has shown in non-control studies interesting results. (55-56) Further research is needed to better evaluate this ancient art in the treatment of the MS patient.
6—Management of acute infections
Acute respiratory tract infections such as sinusitis, colds and flus and acute urinary tract infections must be dealt with immediately with homeopathy and hygienic measures. These are critical times. If they are not attended soon enough the patient may experience a relapse of MS symptoms. Taking the remedy for the chronic state will often not prevent a relapse. If the acute condition is dissimilar to the chronic one and an acute remedy is prescribed the patient will recover quicker and this may prevent a relapse. In certain cases the chronic MS condition still relapses in spite of a quick recovery of the acute condition. The adoption of hygienic measures at such times may make the difference between a severe exacerbation and a good recovery. Rest is a must during a period of acute infection. Hydrotherapy applications will also be very useful in the hands of a knowledgeable physician.
7—Prophylaxis
Before and during the winter months the use of Influenzinum has been shown to be useful for preventing flu and Tuberculinum for preventing common colds. (58-59)Oscillococcinum has also been used successfully for preventing the flu. The prophylactic use of remedies must be individualized in each case depending on various factors such as the degree of exposure, sensitivity of the patient, past history of acute conditions, etc.
References
1. Herndon RM. Pathology and pathophysiology of multiple sclerosis. Semin Neurol 1985;5:99-106.
2. Morse PH. Retinal venous sheathing and neovascularization in disseminated sclerosis. Ann Ophthalmol 1975;7:949-52.
3. Vuia O. The bening form of multiple sclerosis: anatomo-clinical aspects. Acta Neurol Scand 1977;55:289-98.
4. Poser CM. Pathogenesis of multiple sclerosis. ActaNeuropathol 1986;71:1-10.
5. Ormerod IE, et al. Imaging of multiple sclerosis. In McDonald WI, Silberberg DH, eds. Multiple sclerosis. London: Butterworths, 1986:11-36.
6. Vandenbarrk AA. Critical immunologic events in multiple sclerosis: overview and summary. Res Monogr Immunol;7:257-70.
7. Larner AJ. Aetiological role of viruses in multiple sclerosis: a review. J R Soc Med 1986;79:412-7.
8. Govaerts A. HLA et la sclerose en plaques. Path Biol 1986;34:738-40.
9. Ebers GC. Immunogenetics and CSF studies in multiple sclerosis. Res Monogr Immunol 1984;7:233-56.
10. Francis DA, Batchelor JR, McDonald WI, et al. Multiple sclerosis in north-east Scotland. Brain 1987;110:181-96.
11. Martin JR. Herpes simplex virus types 1 and 2 and multiple sclerosis. Lancet;ii:777-81.
12. Warner HB, Carp RI. Multiple sclerosis and Epstein-Barr virus. Lancet;ii:1290.
13. Legac P. Le probleme histo-physio-pathologique de la sclerose en plaques. Bull Aca Sci 1960;250:2299-301.
14. Greisman SE, Wisseman GL. Studies of rickettsial toxins. J Immunol 1958;81:345-54.
15. Jadin Y. Maladies rickettsiennes en sclérose en plaques. Ann Soc Belge Med Trop 1962;42:321-45.
16. Field EJ, Chambers M. Rickettsial antibodies in multiple sclerosis. Br Med J 1970;1:30-32.
17. Legac P. Rickettsial antibodies in multiple sclerosis. Br Med J 1971; 2:341-2.
18. Szekeres J, Palffy GY, Paradi J. Rickettsia specific antibodies in multiple sclerosis. Lancet 1980;ii:1089-90.
19. Legac P, Wullfaert F, Arquie E, et al. Résultats de l’antiobiothérapie à large spectre sur 30 cas chroniques de sclérose en plaques rickettsienne et neo-rickettsienne. Bull Soc Path Exot 1964;57:263-76.
20. Warren S, Greenhill S, Warren KG. Emotional stress and the development of multiple sclerosis: Case control evidence of a relationship. J Chronic Dis 1982;35:821-31.
21. Bamford CR, Sibley WA, Thies C, et al. Trauma as an etiologic and aggravating factor in multiple sclerosis. Neurology 1981;31:1229-34.
22. Bamford CR, Sibley WA, Laguna JF. Anesthesia in multiple sclerosis. Can J Neurol Sci 1978:5:41-4.
23. McAlpine D, Compston N. Some aspects of the nature of disseminated sclerosis. Q J Med 1952;21:135-67.
24. Westlund KB, Kurland LT. Studies on multiple sclerosis in Winnipeg, Manitoba and New Orleans, Lousiana. Am J Hyg 1953;57:380-411.
25. Ingalls TH. Triggers for multiple sclerosis. Lancet 1986;ii:160.
26. Miller JH, Allison RS, Cheeseman EA, et al. Pregnancy as a factor influencing relapse in disseminated sclerosis. Brain1959;82:417-26.
27. Leibowitz U, Antonovsky A, Kats R, et al. Does pregnancy increase the risk of multiple sclerosis? J Neurol Neurosurg Psychiatry 1967;30:354-7.
28. Sibley Wa, Bamford Cr, Clark K. Clinical viral infections and multiple sclerosis. Lancet 1985;i;1313-5.
29. Gay D, Dick G, Upton G. Multiple sclerosis associated with sinusitis: case controlled study in general practice. Lancet;i:815-9.
30. Palffy G, Merei FT. The possible role of vaccines and sera in pathogenesis of multiple sclerosis. World Neurol 1961;2:167-71.
31. Miller H, Cendrowski W, Schapira K. Multiple sclerosis and vaccination. Br Med J 1967;2:210-3.
32. Smith CR, Scheinberg LC. Clinical features of multiple sclerosis. Semin Neurol 1985;5:85-93.
33. Sibley WA. Management of the patient with multiple sclerosis. Neurol 1985;5:134-45.
34. Krieger. Cas de guérison d’une paralysie progressive de la moelle épinière. J du Dispensaire Hahnemann 1862-63;1:240-4.
35. Rorke WW. Results of homeopathic treatment in a well-defined and well-known chronic nervous disease. Br Hom J 1925;25:131-44.
36. Sloan TG. Dissiminated Sclerosis. Int Hah Ass Trans 1926;47:245-7.
37. Spalding RW. Relationship of Plumbum to multiple sclerosis. Hom Rec 1954-55;70:30-8.
38. Tyler ML. Little cases. Homoeopathy 1941;10:332.
39. Hahnemann S. Organon of Medicine. 6th ed, Los Angeles: JP Tarcher, Inc., 1982.
40. Russell WR. Multiple sclerosis: control of the disease. Oxford-New-York-Toronto: Pergamon Press, 1972.
41. Swank RL. Multiple sclerosis: twenty years on a low fat diet. Arch Neurol 1970;23:460-74.
42. Dworkin RH, Bates D, Millar JH, Paty DW. Linoleic acid and multiple sclerosis. A reanalysis of three double blind trials. Neurology 1984;34:1441-5.
43. Cendrowski W. Multiple sclerosis and MaxEPA. Br J Clin Pract 1986;40:365-7.
44. Sinclair HM. Forward. In Field EJ. Multiple sclerosis in childhood. Springfield: Charles C. Thomas, 1980:vii-xiii.
45. Field EJ, Joyce G. Simplified laboratory test for multiple sclerosis. Lancet 1976;ii:367.
46. Seaman GV, Swank RL, Zukoski CF. Red-cell-membrane differences in multiple sclerosis are acquired from plasma. Lancet 1979;i:1139.
47. Mickel H. Multiple sclerosis: A new hypothesis. Perspect Biol Med 1975:18:363-74.
48. Baker RW, Thompson RH, Zilke KJ. Fatty acid composition of brain lecithins in multiple sclerosis. Lancet 1963;i:26.
49. Jensen GE, Gissel-Nielson G, Clausen J. Leukocyte peroxidase activity and selenium level in multiple sclerosis. J Neurol Sci 1980;48:61-7.
50. Mazzella GL, Sinforiani E, Salvodi F, et al. Blood cells glutathione peroxidase activity and selenium in multiple sclerosis. Eur Neurol 1983;22:442-6.
51. Jensen GE, Clausen J. Glutathione peroxidase activity, associated enzymes and substrates in blood cells from patients with multiple sclerosis-Effects of antioxidant supplementation. Acta Pharmacol Toxicol(Suppl) 1986;VII:450-3.
52. Golberg P, Fleming MC, Picard EH. Multiple sclerosis: decreased relapse rate through dietary supplementation with calcium, magnesium and vitamin D. Med Hyp 1986;21:193-200.
53. E.C. (An anonymous homeopathic physician). Poisoning vermilion in dental plates. New Engl Med Gaz 1872;7:69-74.
54. Allen HC. A case of mercurial deafness. Trans Hom Med Soc Penn 1906;43:217-20.
55. Smith MO, Rabinovitz N. Acupuncture treatment of multiple: two detailed clinical presentations. Lincoln Acupuncture Clinic of Lincoln Hospital, New-York, 1987.
56. Steinberger A. Specific irritability of acupuncture points as an early symptom of multiple sclerosis. Am J Chin Med 1986;14:175-8.
57. Schmidt P. Defective illnesses. Calcuta: Hahnemann Pub. Co., 1980.
58. Krishnamurty PS. Report on the use of Influenzinum during the outbreak of epidemic in India in 1968. Hahn Glean 1970;37:225-6.
59. Eizayaga FX. Valor de Influenzinum como preventivo de la gripe. Homeopatia 1973;40:21-2.
——————————————————
Dr Andre Saine
Dean of the Canadian Academy of Homeopathy Dr. André Saine is a graduate of National College of Naturopathic Medicine in Portland, Oregon and has been the Dean of the Canadian Academy of Homeopathy since 1986. He has taught homeopathy extensively in North America and Europe for over 25 years to health care professionals.

The article on “Homoeopathic Treatment of the Multiple sclerotic patient” is a good piece of writng and it reveals that the author went to great pains to present the case.Thank you DR.Andre saine,sir.
Dear Sir
I would like to know where can we follow such treatment in the Middle East. I am from lebanon and my fiance was diagnosed with MS since 4 months.
Dear sir
Your descriptive article was very helpful to understand the disease.
I would like to know till what extent will homeopathy help in treating this disease to a person suffering from it from the past 3years?
what will be more effective at this stage- homeopathy or allopathy?
what are the treatment measures available in India if you can help.
Hoping for a positive reply!
Thank you sir.
seeing ur article; hope for d m.s. pt.is generated i have a pt. in my family hw can i contact u for d treatment.i’m an orthopaedic surgeon in m.l.b.medical college jhansi u.p.india