
Summary:
In my opinion, the common way to make a symptom hierarchy – I mean the selection of symptoms for repertorization – is guided too much by subjective discretion. At the same time, I acknowledge that totally accurate prescribing is not possible within the framework of our rationality. The content of part 1 of this article is how you can still approach the real disease process through logical selection of symptoms.
The starting point of my argument is simple. Illness is an emotional reaction to a cause, which means that the cause and reaction must have an internal connection, which is also reflected in their symptoms. In the case of an illness, there must be a corresponding sensitivity to the cause of the illness beforehand.
This leads to the simple cause-and-effect principle: A specific sensitivity A and a specific causal stimulus B cause an equally specific body reaction C.
Fig.1: A + B = C
So we see three planes (A), (B) and (C). The symptoms of a case are naturally assigned to one of these three planes. The symptoms of plane (A) are all emotional symptoms, i.e. expressions of a person’s emotional sensitivity, the symptoms of plane (B) stand for the stimulus that stimulates this sensitivity, these are the modalities and/or the causal event. The symptoms of plane (C) are the local body symptoms, i.e. the pathological reaction as an expression of emotional dismay.
This means that these three planes (A), (B) and (C) must (shoud) be represented in the form of their symptoms both in the symptom list of an anamnesis and in the repertorization
The problem that now arises is the question, which symptoms of each plane represent the disease center and therefore belong here? This is where logical considerations come into play. Illness is a dynamic process. This dynamic is expressed in the representative symptoms of each of the three planes.
If you examine the symptoms according to their belonging to one of the three planes, it turns out that most of them belong to several planes. I call them combined symptoms. This means that if a symptom of plane (A), which stands for sensitivity, also covers plane (C), which stands for disease reaction, the dynamic relationship between these two planes is covered by this symptom per se. Psychosomatic symptoms, for example, show this connection.
In order to be able to recreate the cause-effect principle with representative symptoms, in order to be able to recreate the cause-effect principle with representative symptoms, it is a matter of reproducing the formula A + B > C with corresponding symptoms that overlap the planes.
In order to be able to recreate the cause-effect principle with representative symptoms, it is a matter of filling the formula A + B > C with corresponding symptoms that overlap the levels.
If you know the respective affiliation of a symptom to planes (A), (B) or (C), you can use this knowledge to recreate the above cause-effect process,
How this has to be done in detail is the content of this article. Essentially, it’s about having to make as few discretionary decisions as possible when selecting symptoms.
I assume that our human ability to perceive is trapped in subjectivity. Everything we see, hear and feel is a more or less strong emotion that we compare within the framework of our horizon of experience. This leads to the problem that much of what lies beyond our horizon of experience – which is very easily the case with other people’s illnesses – becomes a reflection of ourselves. We don’t see reality here, only ourselves. This is a central problem of human cognitive ability and is not limited to working with sick people.
Introduction
On the way to standardizing the choice of symptoms when prescribing homeopathic medicine, I followed logically justifiable laws of the disease process. The aim is to understand the internal relationships between the symptoms based on knowledge of these laws. So I went into a “zone” that is unfamiliar to science and where there is hardly any reference literature. So to orient myself here, I used a cyclical approach.
At the beginning of the 2000s, based on R. DAHLKES’ books that deal with the meaning of symptoms, I decoded the motives of over 500 remedies. This resulted in the book “Materia medica der Motive”. I then used these new remedies motifs to retranslate the meanings of symptoms from the drug rubrics of the repertory. This resulted in the book “Human Signatures” with 6,500 translations of symptoms. In the next step, I went back to my materia medica of motifs and improved them using these newly translated symptom meanings. This is how it went on…
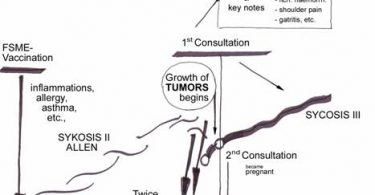
Where diseases come from – disease definition:
Using the example of highly flammable powder (A), onto which a burning match (B) falls and triggers an explosion (C), the planes of dynamics of the disease process can be explained quite well.
A: human sensitivity (inflammation) + B: specific triggering stimulus (burning match) = C: disease reaction (explosion).
The symptoms recorded in an anamnesis, if they belong to plane (A), are symptoms of specific emotional sensitivity. They are all mind symptoms, which is why we will only talk about mind symptoms below.
Plane (B) contains symptoms of the causal plane, i.e. causes and modalities.
Plane (C) represents the symptoms and characteristics of the physical response.
Understanding an illness means recreating this cause-and-effect principle with selected symptoms. To do this, you have to select symptoms from each of the three planes (A), (B) and (C) that fit into this process, i.e. have this inner dynamic and content-related connection beyond all randomness.
Criteria for selecting symptoms in everyday homeopathic life:
• Questions about the timeliness and not timeliness of symptoms:
With repertorization you only use current symptoms. These are symptoms that appeared during the course of the acute illness, most likely as a result of a cause. Symptoms that are older can be current, but are often not symptoms of the current disease process and can therefore relate to other causes.
This does not apply to mind symptoms! As an expression of personality, they can also come from the time before the outbreak of the illness, so they do not need to be current.
• Questions of the safety of symptoms:
In theory, the texts describing the symptoms in the repertory should correspond to the description of the symptoms in the anamnesis!
Unfortunately, there is a language problem lurking here. The meanings of the terms in everyday language depend on the user and change with the background of the event, i.e. the social context. The Zurich homeopath Dr. HEINER FREI speaks of 6% reliable, 32% usable, 62% unreliable, i.e. interpretable symptoms. I see it similarly on an emotional plane.
• The disease process is a reflection of the dynamic relationships between the symptoms:
Imagine a cake made of three large pieces of cake.
Each piece of cake represents a symptom of planes (A), (B) and (C).
However, the three pieces of cake cannot be combined in any way, they can only be put together in the order A, B, C.

Fig. 3:
In order to be able to put this “pie” together, we need knowledge of the affiliation of the symptoms to the respective planes and knowledge of the logic according to which they must be selected in order to reflect the dynamic relationship between the symptoms of the physical reaction (C) and the symptoms of the planes (A) and (B).
A. Criteria of for selecting symptoms as part of a dynamic process:
1. Symptoms as dynamic building blocks:
Assigning the symptoms to the three planes, (A), (B) or (C), produces three simple basic types. Emotional symptoms are assigned as building blocks to plane (A), pure modalities and causes to plane (B) and the pathological body reactions to plane (C).
It is important to remember that many symptoms belong to more than one plane. As an example, a psychosomatic symptom is shown here:
Excitement A causes headache C. So I give it the code AC.
This “AC building block” connects the emotional (A) and reaction (C) planes… what seems to be a complication is actually a simplification. Transferred to the cake above, this AC cake piece is twice the size, so it consists of two parts connected to each other. All that’s missing is the right piece of cake (B) to complete it.
Symptoms as building materials:
a. singular symptoms:
• Plane (A) symptoms: they represent the emotional state of the affected person, their sensitivity, irritability.
• Plane (B) symptoms: They stand for the pressure to adapt from the outside world, ie for the stimulus, the cause or, if this is unknown, the improving or aggravating circumstances (modalities) of the disease.
• Plane (C) symptoms: They represent the body’s disease response as an emotional response.
b. compound symptoms:
• Psychosomatic symptoms have the code AC. They are mental symptoms that cause local symptoms, e.g. Anger A creates stomach pain C.
• Local symptoms C with modalities B have the code BC
e.g.: bending B relieves stomach pain C.
• Local symptoms C can evoke emotional reactions A, ie they are reverse psychosomatic symptoms: code CA
e.g.: Pain (C) causes depression (A).
• Modalities B can cause sensitivities A: code BA. e.g. Darkness B aggravates temper A.
• Emotional arousal A can also evoke a modality B: code AB.
e.g. Excitement A causes menses B. They are rare.
• All three planes (A), (B) and (C) can appear in a symptom: code ABC, BCA etc.
e.g. Excitement A causes abortion BC or bedwetting AC of children B.
You can see that this diversity is reality. The symptoms of medical histories are underlain by it invisibly. Not taking them into account seems to simplify the matter but it has consequences for the quality of the prescription.
In order to use combined symptoms, i.e. symptoms that cover more than one plane, it is necessary to know their assignment to their respective planes. If you know these, the symptoms for repertorization can be put together like dominoes according to this letter code. You can find this information in the ABC file:
ABC FILE http://www.zippermayr-homoeopathie.at/page6.php
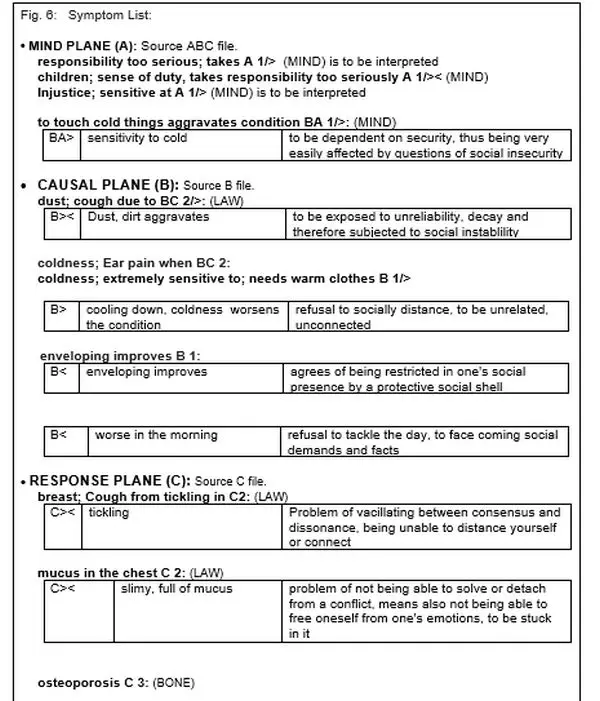
In the ABC file you will find the symptoms described in the following way:
e.g.: appearance; Fear, fear of public A 1/<.
It is a simple plane (A) emotional symptom. The attached number means a ranking according to pathological severity level 1, 2 or 3 (see the explanation of the pathological severity levels in the ABC file).
The direction of the dynamics is indicated here behind the “/” in mind symptoms.
< means defensive, self-centered social dynamics.
> means offensive, communicative social dynamics,
>< indifferent dynamics.
For the procedure that I present in this article (Part 1), you only need the assignment according to capital letters.
Around 2,000 mind symptoms were assigned in the ABC file. They all contain the letter A. The causal and physical symptoms in this file were coded with the letter B or C according to their respective affiliation.
Note: The texts of all symptom meanings can be found on my program, http://www.symptom-sense.com (Google Chrome), which is not translated into English and is subject to payment after 30 days. Each symptom also has two lists attached to it, which can be used to find it in the Synthesis Repertory and the Complete Repertory.
BUT… the analysis method presented here is new and has not yet been implemented at symptom&sense. The program currently offers the current 8,000 symptom meanings. The algorithm according to which it is designed is only part of the procedure presented here, and is therefore no longer up to date.
With these articles, part 1 and part 2, and the attached freely accessible files, ABC, B and C, a subscription to the program is NOT necessary.
ABC FILE: http://www.zippermayr-homoeopathie.at/page6.php
1. It is a symptom lexicon with around 8,000 symptoms, the structure of which follows the KENT chapter division, i.e. mind, organ chapters from head to toe and the general symptoms.
2. These chapters are preceded by the translated meanings of the organs. About 120 in total.
3. Unlike Kent’s classification, the symptoms of each chapter are arranged in the order of plane (A), (B) and (C).
4. The mind symptoms A of all chapters were coded not only as belonging to plane (A) but also according to their dynamics (see part 2 for explanation)..
In addition to knowing the levels to which the symptoms belong, there is a second methodologically important prerequisite:
2. The symptoms of the body level (C) must be synchronous with each other:
What sounds complicated is actually very simple. Synchronous here means in the same direction. If a case has a physical symptom C with modality B , the relationship between the causal plane (B) and the reaction plane (C) is automatically represented by this combination.
In the example case, the cough is due to dust. The cough is the body’s
reaction C and the dust is the cause B. The symptom per se represents thedynamic relationship between these two planes.
Reaction plane (C) symptoms are always physical symptoms. So if you have to add another physical symptom for repertorization, it must come from either the same organ or the same organ system.
In the case of coughing due to dust, this means that an another physical symptom that fits the cause-and-effect formula must belong to the lower respiratory tract.
In the introduction to the ABC file you will find a list in which the organs are arranged by germ layers according to their affiliation.
The disease center – a puzzle of three parts:
Fig. 4: Appearance of the disease center in the cause-and-effect principle: The “?” represents a missing plane that cannot cover the respective symptom. The advantage of combined symptoms is also visible here.
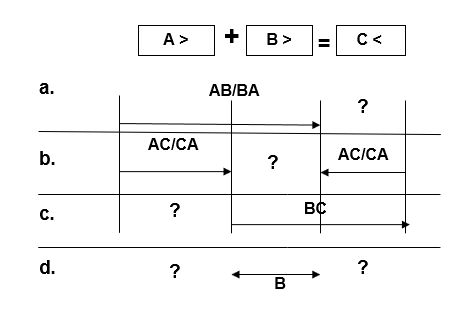
You can see three possibilities for using combined symptoms:
a. AB/BA: Emotional Arousal A + Modality B. Reaction C is missing.
The gap can be closed by supplementing with an appropriate C symptom or an appropriate AC or BC symptom.
b. AC/CA is a psychosomatic symptom. An emotional arousal A causes a physical symptom C. Modality B is missing. The gap can be closed by supplementing with an appropriate B symptom or an appropriate AB or BC symptom.
c. BC is a local symptom C with modality B. The emotional plane (A) is missing. The gap can be closed by supplementing with an appropriate A symptom or an appropriate AB or AC symptom.
d. B here is a traumatic event that will usually be non-specific. This means that no individual sensitivity is required here. Thus, the other planes, which can be AC and/or BC symptoms, determine the analysis.
This ultimately means that in most cases of homeopathic practice you can recreate the entire disease process with combined symptoms.
However, this does not mean that the case can be dealt with mechanically without knowledge of the background events. You only get this understanding through the illness message, the creation of which I explain in Part 2. If you want to do without this, the differential diagnosis must take over the final decision on the remedy.
ad a. Fig. 4 shows the presence of an AB or BA symptom: in practice, for example, this could be a case of chronic stomach problems where anxiety occurs after eating. The ABC file contains:
Anxiety after eating BA 2
A + B = C?
In order to complete the cause and effect formula with a suitable C symptom, we need a BC stomach symptom here,
e.g. Eating makes stomach pain worse BC 2.
By referring to the stomach in both symptoms, BA and BC, the synchronicity condition to the right of = is fulfilled too.
Repertorization Symptoms: Anxiety After Eating BA.
Stomach pain after eating BC.
ad. b. Fig.4: Here we see the value of an AC symptom (psychosomatic) in an example case of abdominal discomfort. The AC symptom must of course be relevant to the case. This means that it must at least affect the gastrointestinal area.
E.g.: ABC file: “Excitement; abdominal pain with AC 2”.
A+? = C
Now it’s about supplementing the missing symptom of plane (B) with a BC symptom from the digestive area in order to ensure the required organic synchronicity too.
e.g. milk; Diarrhea, diarrhea according to BC 2:
A+? = C is thus supplemented by this BC symptom
This means that only simple considerations are required to fulfill the ABC scheme. If symptoms need to be added later for repertorization, all gastrointestinal symptoms are suitable because the same localization means synchronicity.
Fig. 5:
Excitement causes stomach pain AC + milk causes diarrhea BC
Repertorization Symptoms: Stomach pain from anger AC
Vomiting after milk BC
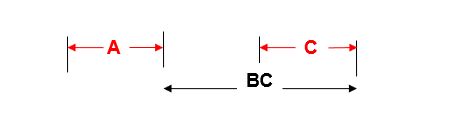
ad c. Fig. 4: The basis of the analysis here is a BC symptom. It is logically complemented by an AB or AC symptom.
ad d. Fig.4: Traumatic cases: A traumatic event does not require specific sensitivity. If the start of a complaint coincides with this, temporal synchronicity criteria apply.
Whatever the complaint is and wherever it is located, if it clearly coincides with the causal event, the event is considered causally posited and all symptoms coinciding with it are considered synchronous.
The resulting psychological and physical symptoms are arranged around the event according to the rules discussed here.
e.g. mind symptoms after head injury BA 3;
Sun; Headache in the BC 2
or
children; Urinary retention in BC 3:
Birth shock, birth trauma BCA 3;
C. The art of patient surveys:
From the examples it can be seen that knowledge of the background to the illness plays a significant role in the result. The symptoms alone do not show the connection gut enough.
As just shown, you should evaluate as little as possible, but at the same time you have to know the background from which the illness arose. The contradiction in therapeutic decisions is that you have to take everything into account and still maintain maximum emotional distance in the case in order not to be reflected by subjective assumptions.
In what I describe as the “ideal” approach, the symptoms are put together like pieces of a puzzle so that they are in the dynamically correct relationship to one another. The picture that the puzzle pieces ultimately form should be underpinned by an idea of the reasons for the illness.
5. PRACTICE – CASE STUDY.
I write the organ references of the case-relevant symptoms in brackets (see ABC file): LAW = lower airways; MIND = mind, TNE = throat, nose and ear area, BLC = blood circulation;
The 47-year-old man is always susceptible to illness from the age of six. He suffers acutely from mucused lungs (LAW) and throat angina (TNE) with painful lymph nodes on the left corner of the jaw. Every year from Christmas to March he is never really healthy.
He is a farmer and even as a child he preferred working on the farm than going to school. It was striking that he justified this with the financial burden on the farm at the time. Even as a primary school child, he had thought he had to make himself useful.
The symptom that children take duty and responsibility too seriously seems to fit here (MIND).
Any type of dust or cigarette smoke will cause extreme coughing fits (LAW). His cough is always triggered by a tickling in the chest (LAW). In general, he also tends to mucus in the larynx and lungs (LAW). Every morning he wakes up hoarse (LAW).
Cold aggravates his being, so he always needs warm clothing. His right ear hurts during the cooling-off phase after showering. Headgear is essential when working outdoors. This also applies to cold air, which causes him an earache without a hood. Cold feet or working with cold meat immediately lead to cold symptoms. Touching ice-cold tools in the workshop is also critical. He doesn’t like going swimming, even 25°C water temperature is too cold. He shouldn’t drink too cold either.
Note: When defining this extreme type of sensitivity to cold, one often encounters a language problem. It clearly seems to be a modality, in fact there is good reason to consider it a CA symptom, i.e. a mixture of emotional sensitivity A and physical characteristic C. These “good” reasons are that the opposite of sensory sensitivity is the loss of sensory sensitivity. This failure of organ function cannot be viewed simply as a modality that aggravates the condition. I therefore view sensory sensitivities as symptoms of the mind (A) and body (C) planes. If you want to know this argued in more detail, you will find it explained in the B file in the chapter, Sensory Sensitivities.
Its strong histamine intolerance (BLC) is remarkable because it seems to have references to dust sensitivity via the term “decay”. Histamine is a protein decay product, its concentration varies with the storage period and the degree of ripeness of the food.
All in all, his life consists of work, he never takes vacations. He says it doesn’t bother him. What upsets him, however, is injustice that happens to him or others (MIND).
As already mentioned, decay is of central importance here, because this term had already appeared in childhood, in the debt of the farm, which, incidentally, he was able to work off after taking over the farm. A few years ago he was diagnosed with osteoporosis (BONE), which he was able to control with high doses of Vit D.
Procedural routine:
Respiratory problems (LAW) have been at the center of the pathology here from the beginning: So the most important symptom is cough from dust BC 2, not only because its localization is the respiratory tract, but also because it has a clear modality.
In order to be able to do this analysis based on an anamnesis, you have to create a list of symptoms of the case using the ABC file, for example on a Word page.
ABC FILE: http://www.zippermayr-homoeopathie.at/page6.php
The same symptoms are then selected from the repertory of the homeopathy program. My radar program has 10 evaluation windows that are arranged one below the other on the left of the screen. The selected symptoms are transferred there, the A symptoms in the 1st window, the B symptoms in the 2nd window and the C symptoms in the 3rd window.
The first look now is at the causal symptoms. You can find them in the 2nd window with the B symptoms. Is there a case-relevant BC symptom that immediately connects planes (B) and (C)?
As mentioned above, cough from dust BC 2 is the case-relevant central B symptom. In order to clarify its dynamic relationships, the dust modality is called up from the B file and transferred to the case record (e.g. Word). As a reminder, the modalities dictate the dynamics even in combined symptoms.
So I put coughing through dust at the center of the analysis.
Since a pulmonary symptom (LAW) was selected with cough, all other symptoms of the lower respiratory tract are synchronous with it.
This applies to coughing caused by tickling in the chest C 2.
This also applies to mucus in the chest C2. All that is missing now is a suitable A symptom. For a better overview, it is now advisable to make a complete list of symptoms.
This also applies to mucus in the chest C2. All that is missing now is a suitable A symptom. For a better overview, it is now advisable to make a complete list of symptoms.
Fig. 7: BC is cough due to dust, C* tickling cought:
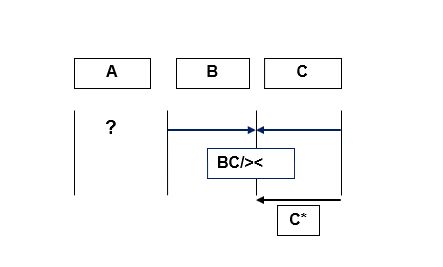
The question mark “?” means it needs a matching A symptom or an AB or AC symptom to close the gap.
In the list of symptoms we see a BA symptom, to touch cold things aggravates condition, with which we could close the gap without further analysis and move on to repertorization. An ideal psychosomatic symptom AC that connects the respiratory system and the emotional plane does not exist.
How to determine the mind symptom that matches the BC symptom, coughing due to dust, is the topic of Part 2 of this article.
What is certain, however, is that the symptoms of coughing due to dust, tickling cough in the chest and coughing due to mucus in the chest can be viewed as a relatively “safe” basis for repertorization:
Fig. 8:
Summe der Symptome – Intensität wurde berücksichtigt
| 1 | BC | dust; cough due to | 45 |
| 2 | C | breast; Cough from tickling in | 69 |
| 3 | C | cough mucus in chest | 37 |
| 4 | BA | to touch cold things aggravates condition | 17 |
| calc. | nat-m. | sulph. | ars. | caust. | cham. | chin. | kali-bi. | phos. | |
| 4 | 4 | 4 | 3 | 3 | 3 | 3 | 3 | 3 | |
| 1 | 1 | 1 | 1 | 1 | – | 1 | 1 | 1 | 1 |
| 2 | 2 | 1 | 1 | 1 | 2 | 2 | 1 | 2 | 3 |
| 3 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 3 | – |
| 4 | 1 | 2 | 1 | – | 1 | – | – | – | 1 |
The remedies of choice are calc., nat-m. and sulph. In the differential diagnosis you can see, that calc. shows a clearly higher sensitivity to cold as the other two remedies . The entire topic, his strong attachment to the house, favors calc anyway.
Calc. LM 3 three granules in 1/4 l water. One sip each (approx. 2 cl) for the first two days. The first day was characterized by a lot of mucus. After a week, all acute symptoms had disappeared, after which he took one sip a week for a while, finally switching to as-needed intake. After three months he called me. He had only needed one sip three weeks ago, which immediately soothed the cough that had arisen.
Note: Calc is one of the large remedies with 13,000 symptoms. There is therefore a good chance that the remedy will not fall through the cracks in the evaluation. Very often, however, the search involves much smaller remediess that are less “friendly” to find. In my experience so far, in the context of this dynamic method, the little ones are often found with only two repertorized symptoms, usually one modality and one characteristic. This is then the input for the differential diagnosis.
Conclusion:
Illness is the key to the reality that surrounds us. The problem with this reality is that we can only orient ourselves in it through our limited ability to perceive. What I mean by this is that we have to classify what we perceive. Hahnemann introduced the three miasms, which over time became five or more. Every classification, including this one, has the flaw of subjectivity. How we can minimize this subjectivity is the subject of this article..
In the ABC file you will find the organs and their translation into their meaning. This is not a classification but serves to understand the disease message.
Symptoms are assigned to organs. We call this localization. It is therefore logical that the message of symptoms can be understood about the importance of the organ. It is shown in a list which organs and organ groups belong together based on their cotyledon affiliation. From this you can derive the relatively simple assignments of organs yourself.
The ABC file is methodologically the most important because the assignment of symptoms to the levels of the cause-effect formula, A + B > C, can be found here. The symptoms for repertorization can be put together like dominoes according to this letter code.
ABC FILE http://www.zippermayr-homoeopathie.at/page6.php
Here you get regular updates and a German version.
This still relatively simple assignment of a symptom to one or more of these three planes is at the center of the procedure. The art of using it in practice is to only get by with these allocations, A, B and C, i.e. to question the patient until the cause-effect formula is fulfilled.
This means that in homeopathy we ourselves, i.e. our subjective perception, and the inhomogeneity of our repertories stand in the way of the dream of therapeutic accuracy. However, you can get as close to this dream as possible through the art of patient surveys within the framework of the cause-effect formula.


Dear Homeopaths
I read this article with great interest. Disease symptoms form in combination the now present image of the disease. Only whatever changed since the beginning of this disease and persists is considered part of the disease-symptom-picture, which upon a medicine is chosen according to symptom similitude.
Mind symptoms as an expression of personality and unaltered since the onset of disease do not form part of the disease-symptom picture, as those reflect the normal character of the patient. here the author goes astray when he writes:
“This does not apply to mind symptoms! As an expression of personality, they can also come from the time before the outbreak of the illness, so they do not need to be current.”
Likewise, the cause of the malady does not form part of the disease-symptom-picture. This means that the bruising and pain,swelling etc. a patient experiences after twisting an ankle, these exact individual symptoms are indicative, yet the cause of those is not.
We find rubrics relating to causes, which are clinical rubrics, ie. Arnica never caused a fall during its proving. Remedies listed there have shown in the past curative, so it may be useful to confirm a selection, however I have cured aftereffects of falls with remedies solely determined by disease-symptom-similitude and not listed in relevant rubrics.
The above two chapters bring me to the conclusion that this new system is of no advantage for the homeopathic prescriber as it,based on a disease theory, mixes unaltered expressions of disease with theoretical deductive thoughts.
For simplicity I refer to C.M. Boger’s little table for arrangement of disease-symptoms:
MODALITIES:
CAUSATION. TIME. TEMPERATURE. WEATHER. OPEN AIR. POSTURE.
MOTION. EATING AND DRINKING. SLEEP. IF ALONE. PRESSURE. TOUCH.
DISCHARGES.
MIND:
IRRITABILITY. SADNESS. FEAR. PLACIDITY.
SENSATIONS:
BURNING. CRAMPING. CUTTING. BURSTING. SORENESS. THROBBING. THIRST
OBJECTIVE ASPECT:
DEMEANOR. NERVOUS EXCITABILITY.
FACIAL EXPRESSION. TORPOR. SECRETIONS. COLOR. ODOR.
PART AFFECTED: Organs. Right. Left.
I completely agree with your comment. There is no need to “philosophize”. Follow the well-established and proven homeopathic path.
The content of the work is the interrelatedness of symptoms in the disease process. This relationship can only be analyzed if symptoms have content. If you can understand this content, you can get information about the prevailing emotional state in the sick person’s body. I think I’m not the only one who believes that illness is the result of a disease-causing cause. From here the logic becomes compelling in that the sick person must be sensitive to the cause in order for a reaction in the form of their illness to occur.
My text is therefore about orientation within the abundance of symptoms of what I believe to be a logical disease process. Especially in Part 1, I show how the symptoms of all levels of the cause-effect reaction are interlinked in terms of content and how they can be put together using this content. In my practice I mainly use the methodology described in Part 1.
The criticism denies the value of the cause-and-effect relationship in the process of illness, but I consider it to be essential. The essence of my text is the selective approach that examines the substantive relationship between the symptom categories of this cause-and-effect formula.
The criticism’s reference to Boger’s categorization misses the point. It’s not about categorization but about the content-related relationships between the categories.