

Prologue:
The central theme of the two articles is the methodology of hierarchizing symptoms for homeopathic repertorization. The current selection criteria are generous, so you have to decide at your discretion or targeted associations. This does not necessarily have to result in incorrect prescriptions. But by discretion I mean the reflection of my personal experience when evaluating other people’s symptom pictures.
In Part 1 of this article, this discretion was largely avoided using the cause-and-effect formula. The principle of the procedure used was:
A specific sensitivity A and a specific causal stimulus B cause an equally specific body reaction C.
A + B > C
The symptoms of a practical case are naturally assigned to one of these three planes. The symptoms of plane (A) are all emotional symptoms, i.e. expressions of a person’s emotional sensitivity. The symptoms of plane (B) represent the stimulus that stimulates this sensitivity: it shows itself in the modalities and/or in the causal event. The symptoms of plane (C) are the local body symptoms, i.e. the physical reaction as an expression of emotional concern.
This means that these three planes (A), (B) and (C) must be represented in the form of their symptoms both in the symptom list of an anamnesis and in the repertorization.
In Part 1 it was shown that the symptoms usually do not just belong to one of the three planes but very often to two, sometimes even all three. If you insert a combined current and case-characteristic symptom into this cause-reaction formula, you have established a connection between two planes without having to evaluate the internal dynamic conditions of the disease center.
E.g.: A case-relevant AC symptom would, if inserted into the formula, mean that only B is missing:
A+B? >C
A current BC symptom of the case (physical symptom with modality) could supplement the missing causal symptom B. However, the prerequisite is that organic synchronicity is present: the C (body symptom) of the BC symptom and of the AC symptom must belong to the same organ or organ system. You can check whether this is the case in a list of the ABC file (it is attached as a link to the article).
Unfortunately, this is not always that easy, which is why it is worth taking a closer look at the dynamic processes in the disease center, which is represented by the cause-effect formula.
1. What to do if the selection of symptoms according to their affiliation to the different planes (A), (B) or (C) is not possible due to a lack of symptoms. It should also be mentioned here that knowing which symptoms you need to enter into the cause-effect formula improves the quality of the patient’s symptom collection.
2. When making the differential diagnosis of the means of choice indicated by repertorization, it is of course an advantage to know the message for the disease. The way to achieve this is shown at the end of this article.
The methodology described in Part 1 of the article uses the assignment of symptoms to their levels (A), (B) or (C). Part 2 deals with the dynamic relationships between these symptoms. Illness is a dynamic process that is reflected in the dynamics of the symptoms involved.
The logic of the internal dynamic conditions in the disease center shows two possibilities:
A > + B > = C <
A < + B < = C >
Left of the =: The dynamics of the symptoms of planes (A) and (B) are each synchronous. This means that they have the same direction according to the criteria mentioned above.
Right of the =: The dynamics of the symptoms of level (C), i.e. the physical reaction, is opposite to the one to the left of the =.
Indifferent symptoms (><) have both directions and can be positioned anywhere. I’ll go into more detail about them later.
Illnesses are therefore an emotional process. This means that the cause-effect event must also have content. This can be, for example, an ambitious person A>, who is prevented from any development by oppressive circumstances B>, which ultimately leads to an auto-aggressive illness C<.
Ambition A> + Repression B> = Autoaggression C<
The symptoms ambition and oppression have the arrow from left to right (>), the symptom autoaggression has it from right to left (<). is therefore oriented in the opposite direction.
For practical work, this means that the dynamic alignment of a singular symptom within a disease process is not random.
This applies to all singular symptoms: If you know their dynamic orientation and their respective affiliation to one of the planes (A), (B) or (C), you must be able to recreate the above cause-effect process with them.
If the A + B > C formula cannot be covered by combined symptoms because there are only individual symptoms that do not allow this, both the dynamic relationship between the symptoms of the different levels and their substantive meaning must be examined.
This is more complex but possible with the help of the free files, B file (causal symptoms) and the C file (characteristics of body symptoms).
Methodology:
The choice of symptoms for hierarchy of symptoms in part 1 of the article was based on the assignment of symptoms to several planes. For this you needed the ABC file. All symptoms that occur within it are in the same direction (synchronous) with one another.
ABC FILE:
http://www.zippermayr-homoeopathie.at/page6.php
In the ABC file, the symptoms are assigned to these three letters, A, B and C. They represent the respective planes to which a symptom belongs. The symptoms for repertorization can be put together like dominoes according to this letter code.
In the prologue to this file, you will also find a list of organs and organ systems. All symptoms that occur within it are in the same direction (synchronous) with one another.
The classification of the symptoms into three levels of severity only plays a minor role. In practice, the more or less dramatic nature of the illness decides anyway.
Emotional symptoms have the following appearance in the ABC file:
Vomiting with (causes) unconsciousness, fainting BA 2/>:
Vomiting is the modality (B) and unconsciousness represents the emotional plane (A).
> stands for extraverted dynamics. Extraverted temperaments prefer contact and react negatively to separation (here with unconsciousness). This becomes clearer when you compare it with the opposite:
Eat; Unconsciousness, fainting after BA 3/<:
Eating means contact. So it must be an introverted, contact-shy temperament (<).
>< stands for indifference.
Menopause: Unconsciousness, fainting in the BA 3/><
Dealing with an inevitable developmental step, here the menopause, is actually absurd and therefore all problems with developmental steps are indifferent.
Approximately 8,000 symptoms are encoded in the ABC file. Body symptoms and modalities have codes made up of B and C and the numbers 1, 2 and 3. In the case of mental symptoms, which are all symptoms that also contain an A, the respective dynamics are placed at the end of the symptom.
B file: http://www.zippermayr-homoeopathie.at/page7.php
I set up the B file for the modalities because here they not only find their dynamics but also their meaning:
| B< | cooling down, coldness improves the condition | desire to distance oneself socially, not bound by references, wants to be separate |
B means that it is a modality, the arrow pointing to the left is, as above, an expression of introversion, i.e. the desire for social decency.
C FILE:
http://www.zippermayr-homoeopathie.at/page9.php
This file describes the properties of body symptoms. Body symptoms are conflict reactions, the dynamics of which are reflected in their properties. This refers to the type of pain or sensation.
| C>< | Tension, tensed, electrically tense | ready to react, having to be prepared, to be hit by a sudden event at any time |
Tension means standing between two opposing forces. It is therefore very easy to understand it as indifferent.
This set of tools can also be used to approach cases that do not follow the procedure shown in Part 1.
As a reminder, I will briefly discuss the analysis methodology shown in Part 1. In the present case, all positions of the cause-effect formula are covered with an AC symptom (excitement causes abdominal pain) and a body symptom with modality BC (milk causes diarrhea).
Fig.1:
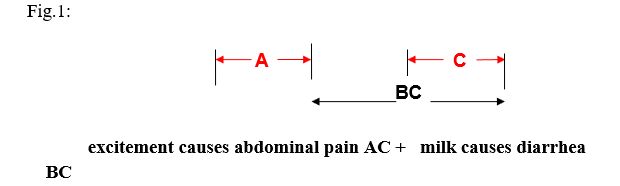
I call cases that can be solved in this way solvable without judgment. This means that you can almost completely refrain from making personal assessments.
What to do in cases that cannot be resolved without judgment?
Note: However, an almost evaluation-free solution is often possible here too.
a.: Missing A symptom: ? + B = C
This is a situation often encountered in practice. AB or AC symptoms are not present. The BC symptom specifies the body symptom C and a modality B.
E.g.: A patient has a stomach problem in which stomach pain is particularly noticeable after sugar.
ABC file: sweets, sugar; Stomach pain after BC 2.
As always, around this BC symptom consisting of modality and location, all symptoms with gastric location C are synchronous and can be used as supplementary symptoms C* for repertorization. So we can add as suitable for repertorization any stomach symptom, preferably a symptom with a characteristic attribute, e.g. burning pain in the stomach.
This means that the analysis situation can be improved even without an A symptom:
A? + B = C + C*
If possible, one repertorizes despite the incomplete situation and hopes that there are already indications of a possible remedy of choice, which can perhaps be confirmed in the differential diagnosis with another characteristic stomach symptom.
If too many remedies of choice prevent this, then not only dynamic but also content-related considerations need to be taken into account. Furthermore, we know that the symptoms of planes (A) and (B) must be dynamically in the same direction (= synchronous). So as part of the cause-effect formula, the BC symptom determines the dynamic conditions.
This dynamic can be found in the B file under “sugar aggravates”.
| B> | sweet, refuses sugar | refusal to experience non-binding attention, to be free from mutual obligation |
A > + B> = C + C*
With this knowledge we can now personalize the case. The rejection or aggravation of sugar means that it is a person who has a problem with non-binding attention and demands commitment towards him
THAT MEANS: The missing emotional symptom A must correspond to the same sense, i.e. have a sensitivity that cannot come to terms with it. The desired emotional symptom A must therefore place emphasis on social commitment and responsibility.
The mood symptoms in the list of symptoms are now examined to see if they fit with this content. It must also be taken into account that the dynamic arrow must be directed to the right, as with sugar rejection: >.
Since it’s clearly about social skills, a possible candidate would be:
ABC file: moral impressions; Mood problems caused by BA 1/>:
In this analysis process, conclusions are drawn from B to A.
b. Multiple causes: A + B? = C
What to do if two traumatic causes exist at approximately the same time. This means that the usual temporal synchronicity in which the onset of the disease and the cause coincide cannot be reliably applied. In addition, there are often several physical symptoms C present, of which one cannot say with certainty which of the two traumas triggered which physical symptom?
In this situation, the properties (accompanying feelings) of body symptoms C become significant. By qualifying the nature of these feelings, a connection to the external cause B can be established.
E.g. A traumatic incident results in numbness in a part of the body as a property:
| CA< | callousness, numbness skin, insensibility, deafness
|
avoiding contact by retreating inwards and escaping the outside |
This CA combination, which indicates a connection between a physical symptom C and the emotional level (A), is a consequence of the logic that extreme touch sensitivity is a modality that also has this connection to the emotional level (BA)
B File:
| BA> | sensitivity to touch, | to be very easily touched by issues of mutual social consensus |
The opposite of sensitivity to touch is insensibility, i.e. not a modality but a property of a physical symptom in which emotional involvement can be assumed.
The characteristic, deafness, is extremely defensive (<) in its dynamics, so the cause (B symptom) should be correspondingly aggressive (>) in terms of content in order to explain this resigned deafness reaction (C characteristic).
This dynamically “convincing” causal symptom B is now sought in the anamnesis.
Let’s assume it’s an accident followed by surgery. Two aggressive influences could be responsible for this deafness:
B File:
| B>< | Injury, hit, fall | Problem of being exposed to an attack, an unrealizable contradiction, not being able to resolve the conflict, only giving up, only being able to signal it as a wound |
| B>< | narcotics, anesthesia intolerant | feeling of not being socially secured, so not letting go of control, not being able to trust in outside help |
You can see that traumatic influences are always indifferent (><), so their dynamics are compatible with both (>) and (<).
This means that if an indifferent A symptom (><) can be found, it decides without us being able to justify it logically.
This could be a mental symptom that is initially incomprehensible here.
Exams; fear, fear of; Exam anxiety BA 1/><:
The question of whether this person’s sensitivity qualified the accident or the anesthesia as a test cannot be answered with certainty. The indifferent dynamics of the emotional symptom, test anxiety, suggests this possibility.
On the value of indifferent symptoms:
I have recently gained the impression that the indifferent symptoms are characteristic of serious cases of illness. The two dynamic directions, < self-centered, away from social contacts and > extraversion towards social contacts, stand opposite each other in states of dynamic indifference (><) and are therefore also an expression of emotional irritation.
This dynamic indifference can most impressively be described as the result of a traumatic event. The cause of the trauma is interpreted by the system (body) as a consequence of its own actions. You must have done something wrong. Action (>) and sequence of actions (<) remain as antipodes in the system. This can remain temporary or permanent as a shock irritation in the system.
It is precisely this indifference that can be easily argued in the case of cancer (adhesions), shock paralysis (paralysis), Parkinson’s disease (trembling) or, in the simplest case, manifested swelling (tumor). It is also plausible that the terms adhesions, paralysis, tremors, swelling can also be attributed to this irritation or indifference.
This raises the question of how these circumstances can be represented in the cause-effect formula.
Ideally, all three symptomatic components are indifferent.
A>< + B>< = C><
Basically, all variants should be possible.
A < + B ><= C > or A > + B >< = C <
? + B >< = C >< or A>< + B>< = ?
In my opinion, these indifferent constellations of symptoms are therefore for serious illnesses such as Cancer of special interest. It makes sense to see the rampant cancer growth as an indifferent phenomenon, i.e. as a loss of social form as a result of a shocking experience in the area of social reciprocity. By this I mean that our entire presence is a social form based on emotional reciprocity. We exist from each other’s existence.
If you explain it dialectically, the following sentence applies: if sensuality means being the object of the sensuality of others (FEUERBACH), then this relation has been lost in the case of cancer. The restoration of this reciprocity therefore corresponds to the restoration of social trust, which is synonymous with the recovery of the social.
PRACTICE – CASE STUDY from Part 1:
I come back to this case study here because all three possible solutions can be demonstrated.
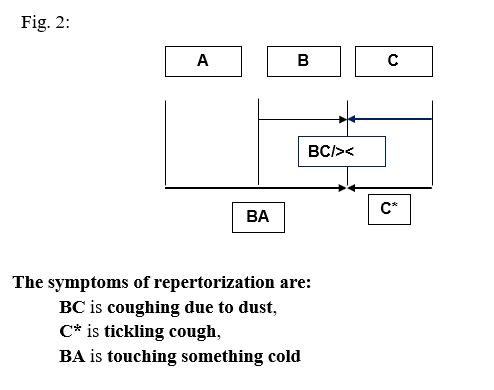
As a reminder: The 47-year-old man is always susceptible to illness from the age of 6. From the very beginning, the focus of the pathology here was respiratory problems and their modality, aggravation by dust.
So the central pathology is cough due to dust (ABC- File: Dust; Cough through BC 2):
B File: http://www.zippermayr-homoeopathie.at/page7.php
| B>< | Dust, dirt aggravates | to be exposed to unreliability, decay and therefore subjected to social instablility |
It is a lower airways (LAW) symptom. The rule that the same body localizations are synchronous and therefore suitable for repertorization now applies to all lower respiratory tract symptoms present in the patient’s history. However, it must always be borne in mind that the more symptoms you use, the more likely you are to overtax the repertory. So it’s always about using as few and characteristic symptoms as possible.
A look at the list of symptoms from part 1 of the article (Fig. 6) also shows that among the physical symptoms listed here, indifference predominates as a dynamic:
ABC File: breast; Cough from tickling in C2: (LAW)
C-File:
| C>< | tickling | Problem of vacillating between consensus and dissonance, being unable to distance yourself or connect |
ABC File: mucus in the chest C 2: (LAW)
C-File:
| C>< | slimy, full of mucus | problem of not being able to solve or detach from a conflict, means also not being able to free oneself from one’s emotions, to be stuck in it |
There is also a corresponding indifferent mind symptom.
ABC File: children; sense of duty, takes responsibility too seriously A 1/>< (MIND)
This list of symptoms allows three solutions:
Solution 1: In part 1 this path was shown in all details.
Solution 2: There is an indifferent mind symptom that comes from the patient’s past but is still active as an expression of his temperament.
ABC file: children; Sense of duty, takes responsibility too seriously A 1/><
The other symptoms in the list above, they are all symptoms of the lower airways (LAW), are also indifferent (><) , so for repertorization we get:
Cough due to dust BC 2:
Breast; Cough due to tickling in the C2:
Mucus in the chest C 2:
Solution 3: Unfortunately, there is no psychosomatic symptom AB or AC. In the anamnesis one finds only singular sensations (A). As already shown, one can draw conclusions about the emotional sensitivity A from the peculiarity of the modality B, here dust. So one tries to explain reaction C, here cough, from the emotional relationship between sensitivity and modality.
To do this, call up the Dust modality from the B file.
| B>< | Dust, dirt aggravates | to be exposed to unreliability, decay and therefore subjected to social instablility |
What follows is a kind of personalization of the disease dynamics. This means that the question arises what sensitivity does a person have to have in order to react to dust by making their symptoms worse?
Fig. 3:
The result of the examination is that the appropriate emotional symptom, which must now be looked for among the symptoms in the symptom list, is about security, stability, security.
His responsibility and sense of duty is based on his fear of decay, so it is relevant to the case and can be added to the repertorization as an expression of his personality… beyond that, in its childish version, it is indifferent.
ABC file: children; sense of duty, takes responsibility too seriously A 1/><
Based on these references, the repertorization of the example case now results:
Fig. 4:
Sum of symptoms – intensity was taken into account
| 1 | BC | dust; cough due to | 45 |
| 2 | C | breast; Cough from tickling in | 69 |
| 3 | C | cough mucus in chest | 37 |
| 4 | BA | to touch cold things aggravates condition | 17 |
| 5 | A 1 | to much sense of duty – children; in | 25 |
| calc. | nat-m. | ars. | caust. | kali-bi. | sep | sulph | zinc. | cham. | |
| 5 | 5 | 4 | 4 | 4 | 4 | 4 | 3 | 3 | |
| 1 | 1 | 1 | 1 | – | 1 | 1 | 1 | 1 | 1 |
| 2 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 2 |
| 3 | 2 | 1 | 1 | 1 | 3 | 1 | 1 | – | – |
| 4 | 1 | 2 | – | 1 | – | – | 1 | 1 | 1 |
| 5 | 3 | 1 | 1 | 1 | 1 | 2 | – | 3 |
The remedies of choice are calc. and nat-m. The discussion of the case history can be found in part 1 of the article.
Finally, reference should be made to the technique of creating an illness message, which can be useful in a differential diagnosis of the means of choice by comparing the illness message and the drug message.
Construction of the background message of the illness:
In general, the question about the personality of the sick person and their emotional conflict should be answered before repertorization so that it can be included in the differential diagnosis.
If we arrange the texts of the symptoms and modalities used here one below the other, we can put them together with the help of the meaning of the pathological phenomenon on the organ:
Touching something cold worsens condition BA 1:
| BA> | sensitivity to cold | to be dependent on security, thus being very easily affected by questions of social insecurity |
Dust; cough due to BC 2:
| B>< | Dust, dirt aggravates | to be exposed to unreliability, decay and therefore subjected to social instablility |
Breast; Cough due to tickling in the C 2:
| C>< | tickling | Problem of vacillating between consensus and dissonance, being unable to distance yourself or connect |
From the ABC file:
* COUGH: Conflict, to be socially isolated having no consensus, but can neither suppress nor openly express his displeasure about this but can only being able to make it audible indirectly.
You can insert the above text elements into the cough text:
The conflict is now exactly named:
Conflict to be dependent on security (BA) but being exposed to unreliability and decay (B)
This is followed by the reaction (cough text), which is expanded with the tickling property:
but can neither suppress nor openly express his displeasure about this, but can only make it indirectly audible (cough), wavering between consensus and dissonance (tickling).
This is the disease message. it describes his emotional state.
Conflict to be dependent on security (BA) but being exposed to unreliability and decay (B) he can neither suppress nor openly express his displeasure about this, but can only make it indirectly audible (cough), wavering between consensus and dissonance (tickling).
Conclusion: Part 1, solution 1 is presented. It relies solely on the ABC file, and here only on the code of capital letters, which takes into account the membership of the symptoms to their respective planes. So the symptoms for repertorization can be put together like dominoes according to this letter code. This procedure has the advantage of using relatively simple coding and therefore has the lowest probability of errors.
ABC file: http://www.zippermayr-homoeopathie.at/page6.php
Here you get regular updates and a German version.
Here you can find the assignment of the symptoms to their respective levels A, B and C. All symptoms that contain an A (emotional level) in their code are also dynamically coded: > (offensive), < (defensive) and >< indifferent.
The fact that the dynamics of the mind symptoms are also encoded in the ABC file and that all organs are translated into their messages only plays a role in Part 2.
In Part 2, this additional information serves the two more differentiated solutions 2 and 3 described above. For this purpose, the ABC file is supplemented by two further files, B file and C file.
B file: http://www.zippermayr-homoeopathie.at/page7.php
Here you get regular updates and a German version.
The B file is about influences whose dynamics can be offensive (>) or defensive (<) or indifferent (><). These influences can be traumatic or provide causal clues in the form of modalities (circumstances of improvement or worsening).
However, this dynamic coding takes place on a linguistic level and can therefore be qualified only as a greater or lesser degree of probability. Its application does not have the methodological certainty of the letter code according to solution 1. So we will only use them if the patient survey does not provide coverage of the cause-effect formula due to a lack of combined symptoms. This forces us to have to deal with the disease message.
This happens by having to draw conclusions from the meaning of an singularl symptom on one plane to the expected meaning of an singular symptom on another plane. Solution options 2 and 3 in the example case clearly show how this works.
C file: http://www.zippermayr-homoeopathie.at/page9.php
Here you get regular updates and a German version
The C file is about the properties of local disease reactions, which are the physical symptoms of an illness. It should be noted here that the dynamics of body symptoms only become apparent through their properties, i.e. the type of sensations, for example whether a pain is burning, pulling, stabbing or whether a feeling is twisting or cramping. Here too, the criteria are offensive (>), defensive (<) or indifferent (><).
Here too, coding was only possible using linguistic probabilities. Therefore, solutions 2 and 3 do not have the security of solution 1.
It turns out that the more you as a person have to involve yourself in the process of selecting symptoms, the more you have to reckon with linguistic imprecision, i.e. the subjectivity of language use.
Be that as it may, the entire examination of the cause-and-effect process in Part 1 and Part 2 of this article demonstrates the process we are dealing with in everyday practice. It is a vagueness that we can only approximate as best as possible using methods that are as objective as possible. Unfortunately, there is no photographic lens that we only need to focus on.


This is beautiful and makes me wonder what other homeopathic treasures we who can’t understand the German language are missing.
Robert Bannan 02.01.24
Comment:
This is beautiful and makes me wonder what other homeopathic treasures we who can’t understand the German language are missing.
Philipp Zippermayr 02.01.24
Dear Robert,
Thank you very much for the kind comment. Regarding the hidden treasures, I would like to point out that I am not a darling of the homeopathic scene in the German-speaking world either.
I am 1. a homeopathic biologist and 2. I am of the opinion that more and more case studies and more and more new remedies will not get us to where we would like to be. Case studies are OK, but trying to imitate them leads to the danger of prescribing based on the name of a disease.
For me, part 1 of the article is what base camp is for mountaineers: a relatively safe base. However, this assumes that the anamnesis has enough characteristic physical symptoms. At the same time the method is very practical. The prerequisite for its use, the coding according to membership in one, two or three planes A, B and C, was relatively safe for me.
Part 2 of the article describes the dynamic situation of illness. That is the good news. The bad news is that encoding according to dynamic criteria, i.e. (>), () or sometimes like this (), or as socially being lifted off, being only related to oneself, i.e. intraverted (<). For me, it wasn't just about coding correctly but also about evaluating all similar symptoms equally across the repertory. This is a Sisyphean task that ultimately cannot be solved. The more you think about a solution, the more it falls apart. As an impulse, the answer is, if he thinks he is noble, he is megalomaniacal. In reflection, however, it can also be an expression of introversion, separation from other people.
I have dynamically encoded all mind symptoms in the ABC file, all modalities in the B file, and all properties in the C file, but do not use this in practice because too many symptoms caused coding problems.
In contrast, the assignment of symptoms to the planes of the causal formula, A, B and C, described in Part 1, is comparatively safe.
In this way you can put a case together like a building block: The ideal case would be the combination of an AC symptom (psychosomatic) with a BC symptom (body location x + modality). Only two symptoms cover A, B and C. Possibly, for repertorization you may also need a C symptom of the same body location x.
If the location C x is characteristic of the case, if it is therefore the complaint for which the patient came, there is synchronicity of the selected symptoms.
If this combination is possible, you are in the inner circle of the disease process and the other modalities in other areas of the body are of secondary (= tangential) value.
However, the normal case in practice is BC (localization C x + modality B) and C (localization C x). You can now repertorize immediately or use file B and file C as described in the article to try to create the disease message from the meaning of the modalities and the properties of the body symptom.
If you have an idea of the illness message that the body communicates through its symptoms, you can use this to infer the appropriate mental symptom A.
You see, I do not agree with Bönninghausen regarding the modalities here, I prefer Kent's view and only use the modalities as pure general symptoms in an emergency. This occurs when a small remedy is involved; for a large one, I require that the modality sought as a combination with the local symptom (BC) can also be found in the subrubrics for the local symptom in question.
For restlessness of the hands, sepia should have "restlessness of the hands" and does not need to be confirmed by the general rubric of "restlessness".
Note: You can require this, but you can't be sure. The pitfalls of the repertory would be a separate chapter.
Finally, I would like to note that I am talking about cases with average symptom patterns. Some cases thwart any strategy due to their lack of symptoms or one-sided selection, so that you have no choice but to rely on keynotes or special symptomes.
So that's my very detailed answer, which is due to your factual comments.
Thank you very much for your kind wishes, which I would be very happy to return.
I wish you and yours also good luck for the coming new year.
Sincerely
Philipp Zippermayr