

Worked out with Boenninghausen’s Concept and Repertory
As a student I have been always fascinated by the various cases shared in seminars and journals, especially life stories, mind symptoms, materia medica, image conceptualization, etc. which used to impress me a lot. During my PG at Dr. M L Dhawale Institute, I came across the rural, tribal area, where we used to work with a variety of clinical conditions. There we encountered limitations in the data we could get from case taking (patients not oriented to homeopathy, uneducated patients). This experience led to a lot of internal reflection. Gradually, after studying cured cases and reviewing old literature, especially of Boenninghausen, Boger, Kent, Phatak, P. Sankaran etc, I got an inspiration and understanding that the limitation in the full data we want, is not always a limitation to treating (one sided diseases and true surgical diseases are exceptions). We should see the case with multiple angles, and find the window to enter, to find the similimum. If the case has a full fledged life history and mind data, Kent’s style of case analysis is preferable. But where, there is limitation or when there is not much striking mental history, we still have scope in Boenninghausen’s and Boger’s concepts.
I’ll discuss the concepts after this case:
CASE:
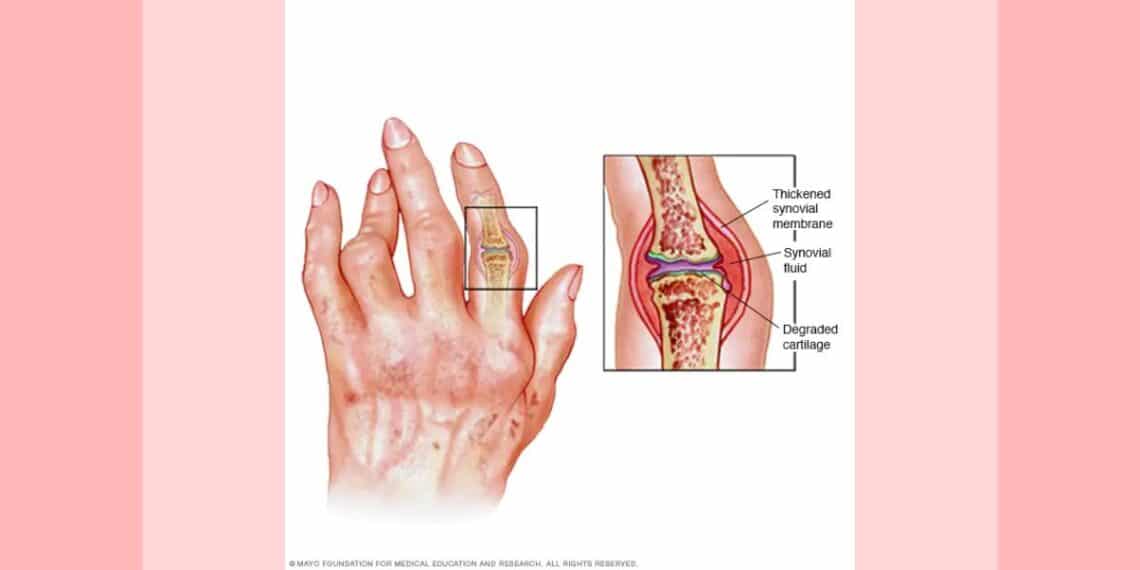
A 34 years old lady from a village, a farming community, economically middle class, complained of pain and swelling in multiple joints since almost one year. The complaint increased in the last three months. She was having pains in both ankles with pedal oedema, more prominent on the left, both knees, finger joints, wrists, lumbar back. The location of pain was shifting. Almost every 2-3 days the pain changed its location except the knee joint pain and lumbar back, which were almost continuous. All complaints worse in the evening, 7pm. On examination there was no marked swelling except pedal oedema. The pain was so severe that she had to take painkillers almost thrice a day, so she could walk (but still there was much pain). She had left much household routine work due to this.
Another complaint she presented, was leucorrhea since 1 year, almost daily discharge; watery, offensive 2+, sticky. Stains but delible.
Occasional irregular headaches.
She was on allopathic treatment with little relief;
Tab Torex(NSAIDs) ½ tab tds
Cap Omez(PPI) OD
Some other data was gathered about physical generals and personal history:
Appetite: poor
Desire: not marked
Aversion: not marked
Thirst: less
Menses: dark red, regular, 25 days cycle. Mild backache during menses.
Sleep: good
Dreams: not marked/significant
Perspiration: scanty, previously used to be profuse.
Thermally: chilly especially after the all complaints started.
Obstetric history: 1 Full term normal delivery, had c/o vomiting all through 9 months of pregnancy
History of abortion in 1st trimester, 2 times.
About her nature I could elicit only little data, she is irritable, likes company. No other significant data or life event was available during case taking.
Investigation:
RA: Positive
Hb: 11.2 gm%
ANALYIS:
Here we have some common data, and unlike a classical case, the mind symptoms and life history are not available with us.
Before further analysis, it is worth looking at some fundamentals of Boenninghausen’s and Boger’s concept.
- Generalization of sensation/location/modality
- Importance of concomitant
This was augmented by Boger with some more points,
- Importance of time modality/factor in disease picture
- Pattern of disease/pathogenesis
- Pathological general; discharges, objective look etc.
Here, general rules of logic and analysis are as it is.
So uncommon is more important always.
TOTALITY:
TIME MODALITY: <7pm
CONCOMITANT: Leucorrhea as a concomitant
(to chief complaints- as started with it, no other obvious cause)
OBJECTIVE DATA- Type of discharge: offensive
General tendency: tendency to abortion
(These were important points in the case which reflected some peculiarity in the case, typical time modality, time association of leucorrhea with chief complaints, general tendency.)
REPERTORIZATION:
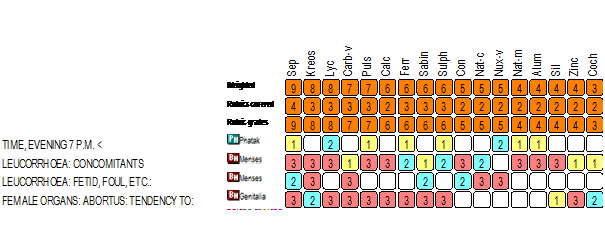
So, on the basis of irritability and H/O vomiting during pregnancy (all 9 months) SEPIA was selected.
PRESCRIPTION:
On 12-03-12
Sepia 200 3 doses given, to be taken in one day with placebo for 2 weeks.
FOLLOW UP:
| After 10 days on 21-03-12 | Pain in all joints better >++Pedal oedema reducedLeucorrhea >++
She reduced the dose of painkiller herself from ½ tab TDS to ½ tab once a day.
|
Rx: Placebo given for another 2 weeks |
| On 6-04-12 | All joint pains were better >++But knee joints and back pain has slightly increasedOedema reduced further, leucorrhea was better >++
|
Sep 200 1 dose given with placebo for 2 weeks |
| On 19-04-12 | She got diarrhea for one day, pains were increased for 2-3 days after dose of sep200Then she was much better, now no more shifting of pains, back pain is also better, leucorrhea almost better >+++ | Kept on placebo |
| On 4-5-12 | Reported with good improvementExcept back pain and knee pain of mild intensityAll other symptoms were gone
|
Rx sep200 1 dose with placebo for 1 month given |
| On 31-05-12 to 26-07-12 | Had 2 episodes of aggravation once after taking onions and once after having “kurkure” which is fast food. They were settled with sep 200 1 dose and 3 doses respectively each time. | Kept on Sep 200 1 dose weekly |
| 10-09-12 | Now much better.She got some pains of mild intensity when placebo is finished.Headache -0-
Leucorrhea -0- Backpain >+++ Knee pain >+++ With some exciting factors like overexertion and some other points she expressed some aggravation
|
Still she kept on Sep 200 weekly for 2 weeks and doing well. |
CONCLUSION:
This case serves as a good example for learning Boenninghausen’s concept and the use of his repertory.
Specific time modality not presented well in Boger’s Boenninghausen repertory, so help of Phatak’s repertory was taken for time rubric. Other rubrics presented well the original idea.
With scanty mental data, and some good understanding of the concept and how to see physical features Boenninghausen is useful in conditions where the typical ‘mind’ style is not adaptable.
The physician has many options to find the simillimum. Each case presents features according its nature, so after genuinely applying all our skills, one should derive the most important and valid data, with minimum subjectivity which would terminate in a good result.
for more detail about RA please visit :



congrats doc. nice case. keep it up.
Well done Doctor.
Since mentals and generals are not many Boger’s approach was adopted. Nothing to comment on this. But we desire to know if the case was followed up with miasmatic remedies subsequently to avoid recurrence. What is the sate of affairs with the patient as on date?
clearing my view about anti-miasmatic; i considered the use of anti miasmatic remedy, but i started with very infrequent doses, and almost each time when there was some recurrence it was effectively relieved with the few dose of same medicine, so still i kept in mind the use of it, and planned to use it when response to same remedy fail or reduced. thanks for valuable feedback.
now she is almost alright and i am planning to keep her on placebo from next follow up.
good work keep going
Nice sharing Navnit. Intelligent use of Boenninghausen Approach and nice result. Keep sharing.
Many thanks for sharing. that was a wright approach to treat a very big illness”RA”
Thanks doctor for sharing your views and case. Difficult to comment as case was incomplete, present status [ as back pain and knee pain continuous at closing the case]. More over due to difficult to collect totality of symptoms [mind, life history or others]- as it is a frequent happening in Homeopathy – from villager, whom the belief is also very less.
Thanks all for appreciating the case and effort,
clearing my view about anti-miasmatic; i considered the use of anti miasmatic remedy, but i started with very infrequent doses, and almost each time when there was some recurrence it was effectively relieved with the few dose of same medicine, so still i kept in mind the use of it, and planned to use it when response to same remedy fail or reduced. thanks for valuable feedback.
now she is almost alright and i am planning to keep her on placebo from next follow up.
anyhow my intention to share the case is to understand the wide applicability n possibility of law of similars.
Thanks.
it is to be brought out whether the patient could be completely cured
very nice case and well presented
many many thanks
for sharing a valuable case….. keep it up Dr….
Hi Navnit, thanks for sharing such a beautiful case.
great job bro……………..
good case… useful tips…
Nice homoeopathic management.
Very good success in our Homoeopathy,But I think more well if it done by fifty milicemale potency.
A good case presentation. Thanks a lot to Dr. Navnit Vachhani.
very nice learning from the case
Thanks for the help in this question.