First published: 16 December 2020 –
Reprinted from: Wiley Online Library
https://onlinelibrary.wiley.com/doi/full/10.1002/ccr3.3674?af=R
Open Access
Abstract
Homeopathic Antimonium crudum may be useful in many pediatric skin conditions if prescribed on symptom similarity. It may especially be helpful in reducing the use of antibiotics and steroids in this age‐group if proven to be effective through larger scientific studies.
1 BACKGROUND
We present three cases of impetigo and one case of bullous pemphigoid neonatorum that benefited from the homeopathic remedy Antimonium crudum, which has a wide spectrum of dermatological applications when prescribed according to symptom similarity. Further larger clinical studies are necessary to establish its role in pediatric dermatology.
Impetigo (ICD 10 L01.00) 1 is one of the most common pediatric skin complaints, caused by gram‐positive bacteria and highly contagious. It may occur as a primary infection of the epidermis or secondary to any trauma or breach in the skin. While the exact prevalence is unclear, it is estimated to account for 10% of pediatric skin complaints. Males and females are equally affected, and it is more common in the 2‐ to 5‐year‐old age‐group. It shows a seasonal tendency and is more prevalent in the hot/humid seasons, that is, summer and fall.2, 3 The Australian aboriginal children exhibited the highest prevalence of impetigo (49%)4
The causative organism is mostly group A streptococcus (GAS) in the nonbullous type and Staphylococcus aureus in the bullous type. Breaches in skin integrity expose fibronectin receptors, promoting bacterial colonization. Self‐inoculation helps the lesions spread further.2, 3 Clinically, these two types show distinct patterns. Nonbullous impetigo often appears as vesicles that coalesce and rupture, and the purulent exudate forms the characteristic honey‐colored crust. The ruptured area exhibits an erythematous base. Rapid spread and satellite lesions can occur, with mild regional lymphadenopathy. Systemic symptoms such as fever are typically absent. The bullous type almost exclusively affects infants. It usually presents as vesicles that form flaccid bullae containing yellow‐ or dark‐colored fluid. This may rupture, exposing an erythematous base and rim. Honey‐colored crusts are not formed in bullous impetigo. Usually, no lymphadenopathy occurs, and fever is a common presentation.2, 3
Malnutrition, diabetes, and immune suppression predispose individuals to the development of impetigo. It is also triggered by other viral infections, such as herpes and varicella, and other causes of skin breach, such as burns, trauma, and insect bites.3
As the diagnosis of impetigo is by rule a clinical diagnosis (as skin swab culture cannot differentiate between the colonization of skin and infection), differential diagnosis must be made between other pruritic lesions common in the pediatric age‐group, such as5
- Herpes simplex virus infection
- Scabies
- Atopic and contact dermatitis
- Varicella zoster
- Cutaneous candidiasis
- Dermatophytosis
- Bockhart impetigo
The characteristic honey‐colored crusts usually signify impetigo and help in differentiating from other pruritic lesions.
Management typically involves topical and oral antibiotics. Approximately 20% of impetigo cases are capable of self‐resolution, and antibiotics have been shown to shorten the disease duration and avert complications that may affect the kidneys, impact the joints, or result in acute rheumatic fever. Without treatment, impetigo will resolve in two to three weeks; with treatment, it will resolve in 10 days.3 Some antibiotic applications have shown that clinical clearance can occur in 5 days and microbiological clearance will occur in 3 to 4 days.6, 7
The second condition, which we present here, unlike impetigo, is quite rare. While the actual incidence has not been investigated, bullous pemphigoid is a rare condition in the pediatric age‐group (ICD 10 L12.0) 1 with just over one hundred cases reported.8 Clinically, it may be diagnosed by the tense blisters with or without underlying erythema and mucosal involvement.9 An immune‐mediated autoimmune disease, it exhibits circulating autoantibodies to antigens BPA1/BP230 and BPA2/BP180 (collagen XII‐NC16A). The initiation of the disease occurs with the IgG recognition of BP180 antigen. Acral involvement of the bullae is a common presentation in the infantile type10 and may be diagnosed by the presence of C3 and IgG deposition in the skin biopsy. It must be differentiated from other bullous disorders such as11
- Epidermolysis bullosa
- Epidermolysis bullosa acquisita
- Bullous impetigo
- Pompholyx
- Linear IgA dermatosis
It usually has excellent prognosis as it responds very well to corticosteroids. The response time varies from a few weeks to a few months, but complete resolution within one year is expected. In 2014, a treatment algorithm was proposed that delineated the approach to mild and severe forms of the disease. The first line of treatment is topical steroids and in case of severe disease, involving more than 10% of the body surface area. A systemic steroid must be introduced, which is withdrawn slowly upon remission. In cases of refractory disease, G6PD deficiency must be ruled out.11, 12
We present here four patients with pediatric skin conditions that were cured by the homeopathic medicine Antimonium crudum. None of these cases were given any conventional medication, and none of them reported any adverse reaction during treatment.
2 CASE SERIES
We present 4 cases of pediatric dermatological conditions that benefited from homeopathic Antimonium crudum. Three of these children had impetigo, and one had bullous pemphigoid neonatorum. These patients were treated by homeopathic physicians in Ukraine.
2.1 Case 1
A 7‐year‐old Ukrainian boy presented on 7/6/2015 with rapidly spreading lesions on the face, nose, and arms. There was a crack in the left nostril (Figure 1). The lesions seemed to be impetigo. This occurred after swimming and diving in a cold pool. In one day, the left nostril was completely blocked with honey‐colored crusts, which became hard‐like stones, with pus discharging from the skin below both nostrils. More small foci appeared on the face and body.
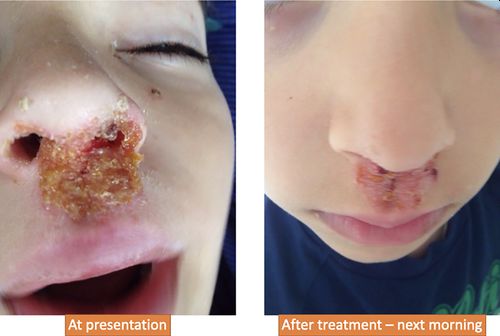
Figure 1
Case 1 presentation and treatment result
2.1.1 Diagnosis
The diagnosis was made by clinical features and the parents called the homeopath.
2.1.2 Differential diagnosis
Bullous erythema multiforme and herpes simplex virus (HSV) infection.
Unlike impetigo, bullous erythema multiforme tends to affect the extensor surface of the extremities and in HSV, usually, there are prodromal symptoms which are absent in impetigo.13
2.1.3 Prescription
The first prescription was Mercurius solubilis 200C, which had no effect. Then, one dose of Antimonium crudum 30C was given.
2.1.4 Follow‐up
The next morning, all small crusts disappeared from the face and nose, greenish nasal discharge appeared, and large crusts started bleeding. Antimonium crudum 200C was given, and in one day, all lesions healed.
2.2 Case 2
A 5‐month‐old Ukrainian male infant was brought to the homeopath with skin eruptions diagnosed by the dermatologist as impetigo (streptodermia) (Figure 2). The eruptions appeared at the age of 3 months in May 2014 during a cold after hypothermia, first on the chin and cheeks, then on the neck and back of head, then on hands, nates, genitalia, and heels. The eruptions were periodical, with eruptions appearing every 2 weeks. There was a cyclical character of the lesions as well, appearing successively as vesicles, ulcers, crusts, and desquamations (Figure 2). The boy was calm and smiling during the day, only crying when being washed with cold water. However, during the night, he was very restless. The period of the aggravation of eruptions was accompanied by constipation, vomiting after nursing and thick, abundant saliva. The eruptions were aggravated after bathing. The tongue was covered with thick white mucus. No conventional treatment was given.

Figure 2
Case 2 presentation and treatment result
2.2.1 Diagnosis
Clinical diagnosis based on presenting features was made by the homeopathic physician.
2.2.2 Differential diagnosis
Pemphigus vulgaris—while the lesions were extensive, the mucous membranes were not affected as happens in pemphigus vulgaris. Pemphigus foliaceous is a close mimic but usually appears in the adults.13, 14
2.2.3 Prescription
On 20/7/2014, Antimonium crudum 12C once a day was prescribed.
2.2.4 Follow‐up
After 3 weeks, the mother noticed that the usual 2‐week cycle of the eruptions did not appear. The remedy was stopped.
After 2 months, the skin became clear completely. The child had no problem with the skin during the 6 years of follow‐up.
2.3 Case 3
A 6‐year‐old Ukrainian boy presented with skin eruptions. The boy often visited a swimming pool with heated water, but on one occasion, the water was cold. After a few days of bathing in cold water, a wet spot appeared inside the right hand with small pimples. Many vesicles appeared on the face, body, and arms, which opened with sticky discharges forming thick yellow crusts (Figure 3).

Figure 3
Case 3 presentation and treatment result
Diagnosis: was made based on clinical features by the homeopathic physician.
Differential diagnosis: Similar to Case 1, this case must be differentiated from bullous erythema multiforme and HSV infection. The appearance of honey‐colored crusts on face and the absence of prodromal symptoms pointed to the impetigo diagnosis.
2.3.1 Prescription
Graphites 30C was prescribed on 10/9/2014, and Graphites 200C was prescribed on 11/9/2014. The skin condition worsened; some large blisters appeared on the forehead, finger, and arms. Severe eruptions appeared around the eyes and under the right arm. He could not open the eyes or raise the right arm. The eruptions were itching with burning. The child peeled off the crusts during night sleep and was very irritated. The area under the right arm looked as if scalded and was very painful. New vesicles appeared on the left arm.
On 16/9/2014, Antimonium crudum 10 M was given.
2.3.2 Follow‐up
On 17/9/2014, the spreading of eruptions stopped, itching subsided, and moist eruptions dried and developed crusts, which detached without discharging. The face was completely clear.
On 20/9/2014, only light crusting on left upper limb and armpit remained; other areas were clear.
On 27/9/2014, all skin eruptions disappeared, and the skin became clear.
2.4 Case 4
A 10‐day‐old female Ukrainian infant living in the USA with bullous pemphigus neonatorum was seen by a homeopath. On the 7th day after birth, yellow blisters appeared in the left armpit, which then opened and became wet on the surface with a yellow sticky discharge (Figure 4).

Figure 4
Case 4 presentation and treatment result
Diagnosis: In the hospital, the patient was diagnosed clinically with “bullous pemphigoid neonatorum” (BP), and immediate introduction of intravenous antibiotics for sepsis prevention was recommended. No immunofluorescence investigation was conducted, which would have been desirable to confirm diagnosis.
Meanwhile, patients consulted the Ukrainian homeopath via video consultation. The infant had thick white mucus on the tongue that was similar to candidiasis. The general condition, sleep, and appetite were normal, and the baby was not vaccinated.
2.4.1 Differential diagnosis
Established clinical criteria for diagnosis of childhood BP are by appreciating the tense blisters with or without the underlying erythema or mucosal involvement. Appearance of blisters and urticarial plaques on the trunk with tense blisters on acral sites is the characteristic of childhood BP.8, 9, 11
The main differential diagnosis is bullous impetigo which does not exhibit urticarial plaques as in BP. Epidermolysis bullosa may be difficult to diagnose clinically but usually requires minor traumas for the lesions to appear and has a much more severe disease course than BP.
The homeopathic treatment was started before the introduction of antibiotics.
2.4.2 Prescription
One dose of Antimonium crudum 30C was given on 30/3/2018.
2.4.3 Follow‐up
Immediate changes were appreciated, averting the need for antibiotics.
On 6/4/2018, purulent discharges were completely reduced, and no further spread of eruptions was observed.
On 13/4/2018, all skin eruptions disappeared, but some pigmentation remained.
On 8/8/2020, the child was clear of the complaint with no relapses so far.
3 DISCUSSION
Classical homeopathy approaches any condition in a holistic, individualized manner. This means that it takes into consideration the hereditary predisposition, circumstantial stress, diseases suffered in the past, immune response characteristics, drugs given, responses to these drugs, and the current diagnosis with detailed symptomatology to choose a remedy.15, 16 The homeopathic pharmacopoeia includes many drugs that have an action predominantly on the skin,17 and many disparate conditions have shown excellent response clinically to them.18–21 Nwabudike in 2016 published a homeopathic case report of impetigo in an elderly man 22 who benefited from a different homeopathic medicine, Hepar sulphuricum.
Antimonium crudum, the black sulfide or native sulfide of antimony, is another such medicine that has an effect on skin conditions,23, 24 prepared homeopathically according to Class VII of Indian pharmacopeia.25 Homeopathic proving of the remedy has produced many clinical symptoms that indicate its relevance in impetigo and other dermatological conditions. Pustules with inflamed red base, sensitive to touch is an indication of antimonium crudum23 that is akin to impetigo and bullous diseases. The semiotic similarity between the symptoms produced during proving of Antimonium crudum and those produced in the patient gives us the indication about which dermatological conditions the medicine will be serviceable homeopathically in.23
While pharmacological action of homeopathic remedies remains to be proven, Antimonium crudum has been shown to be beneficial in murine leishmaniasis through a distinct promotion of B‐cell activity.26, 27 The medicine exhibited immunomodulating activity where it promoted Th1 predominance and helped control the infection process.28 Th2 cell‐associated cytokines are shown to be involved in pathogenesis of BP,29 and promotion of Th1 by the homeopathic medicine may be a way of switching to efficient inflammatory response, leading to resolution of the disease. B‐cell activity is shown to be crucial for the effective clearance of infections30 and also for the formation of effective antibody memory,31 a probable mechanism by which the homeopathic preparation Antimonium crudum is effective in common dermatological infections such as impetigo.
In the cases we have presented, the first three were infections, and the last one was an autoimmune condition. The indications for homeopathic medicine, however, do not stop at diagnosis. The same remedy may be indicated in infections or autoimmune conditions because of the other associated symptoms, especially those that do not seem to be a direct consequence of the pathology. For example, patients requiring Antimonium crudum usually have a very thick milky white coating on their tongue. They also have an unexplainable craving for cucumbers and pickles.23, 32 The common line running in the above cases was aggravation at night and aggravation from cold bathing. Such peculiarities may seem insignificant, but to homeopaths, they are of paramount importance. The idea is that in a diseased state, it is not just the local organ or system that is affected but rather a general affection occurs, altering many faculties of the being. Considering this entire profile alone indicates the right medicine. This idea is no longer far‐fetched, as studies show the systemic nature of inflammation, immune response, and sickness behavior.33, 34 While these are being studied in a generalized manner by conventional medicine to understand the common changes in the whole spectrum of disease, homeopathy considers these changes at the individual level and has treated so since the last two centuries. In these cases, such an approach was proven to be beneficial.
4 CONCLUSIONS
The homeopathic medicine Antimonium crudum was beneficial in the four cases of pediatric skin conditions presented here. Antimonium crudum may help in reducing the antibiotic exposure in children with dermatological conditions, a welcome development in this era of antibiotic resistance. The relevance of this drug in homeopathic potencies to dermatological conditions needs to be investigated further with scientific studies.
ACKNOWLEDGMENTS
Published with written consent of the patient.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.
AUTHOR CONTRIBUTIONS
TK and NK: were the primary physicians who treated the patients, obtained the data, and analyzed them for the study. SM: wrote the manuscript and obtained the references. GV: was the guide, final approver, and guarantor of the work. All authors have read and approved the final version of the manuscript.
STATEMENT OF ETHICS
Ethical approval was not sought as the report is from treatment results and not a trial. The patients’ parents were explained about the publication, and they have provided written consent for publication.
CONSENT FOR PUBLICATION
Written consent was obtained from parents for publication of their wards’ case details and photographs.
© 2020 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
This is an open access article under the terms of the Creative Commons Attribution‐NonCommercial‐NoDerivs License, which permits use and distribution in any medium, provided the original work is properly cited, the use is non‐commercial and no modifications or adaptations are made.



Kent chela AH Grimmer mentions dulcamara as specific in IMPETIGO,yellow crusts turn brown hue,homoeo recorder sep 1952 refers.