

The goal of this article is to give a broad overview on Cycles and Segments philosophy as well as to shed light on some of the more day-to-day aspects of using Cycles and Segments in practice. Paul Herscu ND originally described this way of thinking in the early 1990’s and continues to distill and refined Cycles and Segments with the help of many of those we have been fortunate to teach. I have been using the Cycles and Segments approach to case taking and case analysis for the past fifteen years and have been teaching the material just about as long. I find the internal consistency and focus it affords, helps me organize so much of homeopathic knowledge and streamlines my practice, ultimately helping my ability to help my patients.
I did not start out using Cycles and Segments after my naturopathic school homeopathy training. Like many loving new wives, I was at first resistant to any ideas that Paul had! Trained in the 1980’s, I was, as many a classical homeopath, prescribing most often on pattern recognition; I was always hoping for that “feeling” with patients when I was most certain I had found a remedy that would help. The problem with pattern recognition was that sometimes there was a pattern I did not recognize or worse, I thought I did, yet the remedy did not work. And when it came to teaching, the arbitrariness of that approach did not suit me. I was teaching rudiments of materia medica and the repertory and passing down philosophy as I had been taught, but I grew increasingly dissatisfied. The further I went into practice and into teaching, the more I craved an approach that would unify homeopathic knowledge, that would be logical and eminently teachable. The philosophy of holism was so wonderfully spelled out and eloquently described by our forebears and I, like many before me, could do an adequate job in passing that philosophical part on, yet the practical tools of our trade seemed far from that elegance, at worst reductionistic; the implementation did not echo the beauty of our philosophy. Add to that, the learning curve was just too steep; I knew the profession was loosing many bright potential practitioners because it was unscientific, there was too little structure and predictability and not much assurance that remedies would work. Some grabbed onto particular philosophies or other natural medicine approaches, the truly disillusioned, left.
As Paul formulated his ideas about Cycles and Segments and taught other teachers, colleagues, students and peers, myself included, and received feedback on what worked and what did not, we could both see that the benefits of this unified, organized and always-applicable-to-every-patient approach were going to run deep. Finally we could tell when we were done taking a case. Finally we could see how all the unusual or characteristic symptoms fit into the patients’ stories. Finally we could tell which were the important symptoms in the case, i.e. which minutiae we should pay attention to. And finally, we could understand what the remedy given should do for the patient. The randomness was lessened, the accuracy was improved and ultimately, the patient outcomes were better. When Paul, with help, put the philosophy and practical application into a computer program (the Herscu Module on RADAR) the ability to use Cycles and Segments in the office, with the patient present, became a reality for many. We knew by then we had something that was at once teachable, transparent and relatively easy to master. We could take a frank beginner and in a solid couple of years of dedicated study, have them able to take a cogent, organized case, correctly analyze the information gathered from the patient’s story, from their own observations and perceptions, repertorize with skill and direction, and come up with 6-10 possible remedies or so. This is the right direction for our profession. From there, even most beginners can cross off 2-3-4 remedies and then move to comparative materia medica to help inform their decision on how to choose the best possible remedy for the patient. Also there would now be a short list of other possible remedies to consider at the time of the first follow up visit and the homeopath would not be starting from square one. We have now taken hundreds of students through the process of learning Cycles and Segments. Some were seasoned prescribers, others brand new to the profession. We continue to take and integrate feedback on this approach.
Nothing in homeopathy is easy, but it should not be so daunting that it turns away dedicated and well-intentioned providers. By training small groups at first and by creating a supportive network of alumni, we aim to give those who use Cycles and Segments a community in which to practice. The Internet has been helpful in this regard, our alumni Listservs are used often for help with cases, getting feedback, asking about rubric selection and philosophical questions as well as sharing some of the small wonders of homeopathic practice. Our highest goal is that ultimately, our patients will benefit from accurate prescribing and that the potential of homeopathy will be realized. We also keep as an ongoing objective that those who offer care will relish a challenging but not overwhelming job; we love when any homeopath works hard, feels engaged, inspired and also satisfied in work well done.
In this article I will share a case and illustrate how to apply Cycles and Segments to a typical patient in practice. While I am taking the case of a patient, I create a Cycle of the patient’s complaints. A Cycle is made up of group of Segments. A Segment is a group of symptoms that represent the same idea. Below, I will describe the computer program I use to assist me, but the underlying philosophy and approach can be utilized without any computer software as well. With each symptom a patient shares, I think to myself, what is that symptom an example of? And are there other examples in their story? I not only think that question, I pose it to the patient or parent of the patient. My orientation is to hear complaints with this understanding. As I am observing patients, their dress, posture, body language, all the kinesthetic elements I also use in casetaking, I am perceiving those things in context, too. For instance, if I have a patient with abdominal bloating, I would ask what is that an example of? Perhaps it is an example of fullness and swelling. Perhaps they also have swelling around the eyes or swollen ankles. I would put all these symptoms in one Segment as they represent the same idea and then I look for the best rubrics to represent these specific ideas. I would call the Segment : “Swelling.” Sometimes we see Segments that include physical body and mental or emotional concerns, too. In a section called swelling, if it applied, I might also use a rubric like Mind, Haughty. On the other hand, if there was abdominal swelling that was quite firm, I might see that as an example of “hardness,” and would wonder if there were other examples of “hardness” in their story, such as hard nodules in the glands, or tendency for forming hard stools. Perhaps the person was also very shut down emotionally- all examples of hardness. So conclusions about understanding any particular symptom, i.e. to make a generalization about a Segment, are always context dependent and as such, rely strongly on what else is going on in the patient’s story. You cannot predict the way any symptom will fall within the context of the person’s life, but you can make observations and you can have those observations inform your questions.
In another case, if I had a patient with tremendous discharge, say chronic loose stool or excessive nasal mucous and they also had issues with anger outbursts, I could put these seemingly disparate symptoms and their related rubrics in one Segment and I might call that Segment “Discharges.” In this way, no symptom takes on disproportionate measure and I am sure that I am looking at the overall tendencies of the patient. I no longer worry that I will not perceive or remember the exact correct rubric, because I am understanding the whole concept of the patient’s pathology. I can also trust that the remedy that will prove helpful to the patient will come through the repertorization. In this way Cycles and Segments liberates the homeopath. We can move away from the striving for perfection and in so doing, do a better job for our patients.
The Herscu Module on the RADAR computer program that reflects this approach is straight forward to use and with most all my patients, I repertorize on my laptop as I am taking the case. After an initial period where I work hard to connect with the patient, which includes explaining my approach a bit if they are interested, (I send most new patients a copy of my CD What Every Homeopath Wants Her Patients to Know*, before our first visit) I can be found clicking away as we speak. I am not saying it is easy to do this; i.e. take the case, stay connected to the patient and grounded myself, group symptoms accordingly as they are coming at you, think about rubrics and how to organize them, take adequate written notes AND use the homeopathic software. But as a long-time and competent “multi-tasker,” I love it! Like many others who have come along on this strange ride of becoming computer literate, it is reminiscent of playing a musical instrument. The computer becomes a kind of outgrowth of my thinking. When I had my very first computer in 1986, it was large and took up half my desk and I was awkward with it. Sitting beside or behind one of those behemoths and having to look as I typed interfered with my case taking and I felt some patients feel alienated. But now, as many of us and our patients have computers on or nearby through much of the day and have developed some facility with the tool, patients do not seem to mind. But if that does not work for you, not a problem! Take the case and repertorize afterwards. The most important thing, before you let the patient go, is that you understand the patient, understand all their symptoms, the modalities, the physical generals and most importantly, be sure by the end of your time together you understand what makes that patient tick, what drives their behavior, what most limits them. Grasping their nature, personality wise and their interests, likes and dislikes will all be helpful, too. If you understand all that, as opposed to just an elongated laundry list of problems and modalities, you will be well on your way to finding a remedy that can help.
One advantage of repertorizing while you go, is that you can see what remedies are coming through the repertorization and then you can ask questions that help to rule in and out those remedies. If this occurs during “the flow” of the interview it might take you in new directions with your conversation, as opposed to say, asking yes and no type question by phone or email at a later date to rule remedies in or out. When using a Cycles and Segments approach we see all symptoms in relation to all other symptoms; in this way everything about the patient is related, we lose those long lists of symptoms and issues and instead see the patients as they are: one person expressing imbalance in the characteristic way they do.
Like any skill set, when we teach, we break down all the pieces and encourage our students to gain expertise in each of the component areas. We separate out all the different elements of getting the story, the verbal part, the family history, the history of the present illness, the modalities, the physical generals and the mental and emotional aspects, etc. One needs to be able to take a case backward and forward and with the eyes closed, so to speak. Knowing these questions and knowing them cold and knowing them enough so that when interesting stories come up you can go on that tributary with your patient, but then just as capably you can bring the case back to center afterward, that is what we are going for. I have watched far too many homeopaths while taking a case, hear a story, perhaps it is a tangent, perhaps it is a very essential part of the case, but regardless, the homeopath loses their way. With Cycles and Segments, because we are trying to understand the cycle of the patient’s pathology, we stay more focused in casetaking. We are looking to close the Cycle with each patient and understand their symptoms in context. When we teach case taking and especially consistency in case taking for both the first visits and follow-up visits, we encourage our students to strive to make this information-gathering second nature. Paul has a wonderful picture of Greg Louganis hanging over his desk in our clinic.
There is below the photo of him in a perfect pike position the following quote:
I am a real perfectionist. But that’s the irony. In order to do it perfectly, I have to let go of perfection a little. For instance, in diving there is a sweet spot on the board right at the end. I can’t always hit it perfectly. Sometimes I am a little back from it, sometimes a little over. But the judges can’t tell that. I have to deal with whatever take off I have been given. I can’t leave my mind on the board, I have to stay in the present. I have to be relaxed enough to clue in to the memory tape of how to do it. That’s why I train so hard. Not to do it right, but to do it right from all the wrong places.
What this quote says to me is that you need to be able to be “in the zone” when you are taking a case. You need to be unflappable regardless of what the patient says or does or what else is going on in the room with children, toys, noise etc. When your individual casetaking and case analysis skills are sharp, you are less likely to be pulled off the goal by things in the interview that are distracting. The more the elements of case taking that are automatic, the better you can do this. To make case taking automatic, yet also responsive to each individual patient before you, understanding the individual pieces of the case taking process and practicing them is essential. When we teach, we break down all the parts for our students and then make them do the work of learning and of practice. I will not go into each of those pieces here, as it is outside the purview of this article but all elements are describable, teachable, practicable and improvable!
We spend a good long weekend explaining our philosophy and how we apply it and through years of study together, the philosophy and understanding is further elucidated. We spend sufficient time early on teaching the rudiments of the repertory. We describe the history and basic layout of the repertory and overarching concepts of the language; we then go section by section with repertory exercises so that all students develop facility with finding symptoms. Part of being able to utilize this already difficult tool is having familiarity with its idiosyncrasies and archaic language. This makes the repertory a less intimidating tool and one that is actually useful in practice. Repertorizing using Cycles and Segments thinking offers fewer pitfalls and more safeguards to prevent the discouraging aspects of repertorizing which can occur whether done by hand or computer, i.e. not enough remedies come through or too many remedies come through, or rare and likely not-effective remedies show up.
One of the things Paul is hard at work at is writing the materia medica from a Cycles and Segments perspective so that when looking to possible remedies for patients, we can refer to this more dynamic materia medica. To date he has written the materia medica to over 220 remedies, (many of these are available through the Herscu Letter, (visit www.nesh.com for further info) and indeed that is what we teach when we lecture on materia medica to our students. Many remedies share certain Segments. For instance both Baryta carbonica and Thuja share the symptom of Conscientious about Trifles—but what leads them to that conscientiousness are different things—and what the conscientiousness leads them toward is also different. So, if only one symptom is focused on, you could give either remedy, but by understanding the symptom in context, we are less easily confounded. That some remedies share Segments is also helpful in understanding how patients might move from one remedy to another, but that is out of the realm of this article!
In order to perceive the Cycles and Segments of a remedy, we study cases of those who have been helped by a remedy; we look at the repertory and which rubrics a remedy is found in, and of course we study previously written and understood aspects of a remedy. We have had students in small groups and also on their own come up with Cycles and Segments by reading materia medica in a number of sources. By seeing which symptoms come through a remedy, and which are repeated on many levels across systems, we are honing the same skills necessary in case analysis. When we have conducted provings and have seen which sensitive provers manifest the same kinds of symptoms, again we are applying our understanding of Cycles and Segments.
I should say here that Paul Herscu, my partner and husband extraordinaire, and ongoing teacher, has brought tremendous light and vision to this work. His guidance to myself as well as thousands of homeopaths around the world allows our work to shine. What Paul brings is a kind of clarity to all he does; to watch him with patients as well as with students, which I often have the opportunity to do, there is a kind of magic that happens. But it’s not any inborn kind of magic, it’s not based on intuition or luck. It’s the magic born of hard work and years and years of dedicated study. It’s the magic that can come when the hard labor has been done and the attention is fixed. Because I not only practice and teach with Paul, but also live with him and have raised three delightful teenagers with him, I know his dogged determination and unwavering drive to understand. Understand what? Just about anything that catches his intellect or imagination. So with homeopathy as one of those main areas of interest, Paul does not rest in pushing his own perceptions or his ability to synthesize knowledge, experience and insight or in his ability to articulate for others what it is he is doing. When you watch Paul take a case and see his mind going through all the thousands of cases he has read in old journals, through the veritable bank of patient images, to his lucid understanding of a patient’s nuanced symptoms and expressions and how they fit together, you cannot help feel inspired. I have digested much of what Paul does and do a reasonable job at it myself; I have added to the work perhaps most by bringing my own sensibility to it, by my ability to explain it further, to take people from an old way of seeing things and describe how I made a gradual transition to Cycles and Segments. I am able to make more accessible the ins and outs of this approach to those who are interested and perhaps in some ways I am more approachable than Paul for those with questions. But do know that the underlying philosophical understanding that drives Cycles and Segments is Paul’s work alone, perhaps as an outgrowth and evolution of old masters like Hering and Bonninghausen. My insights are from using it, seeing how I could improve it for my own use and in my ability to teach and make it adoptable by others.
We often see symptoms in the physical and emotional spheres that mirror one another, as the vital force manifests imbalance in similar ways throughout the system. I organize my patient’s symptoms accordingly; seeing how symptoms on various systems and levels are similar helps me to receive a case without being overwhelmed by what might otherwise be understood as separate and distinct problems. I think many a practitioner becomes weighed down by minutiae and looses the big picture of what is going on. Though details are important to the homeopath, we should always be more interested in the general tendencies of a patient. I frequently admonish my students, DO NOT overindulge in those strange, rare and peculiar symptoms! DO NOT build a whole case around a single particular symptom. Now, if a SRP happens to fit into one of your Segments and is part of the case in that way, fine! Use it, Grab it, Don’t be shy, but be sure you see that symptom or characteristics echoed somewhere else in the case before you become side-tracked.
Now on to the case. My observations and thoughts about the patient I will describe are in italics. Whenever I make any observation with a patient I strive to understand what it means. It is not enough to notice things, we need to understand the context and what it means for the individual. So much of what we do as homeopaths, especially after years of practice, is relegated to the unconscious mind. Teaching and writing about homeopathy makes me ever conscious to the fact, that if I really want people to understand what it is I do, how I think, how I analyze a case, how I prescribe- that I need to explain it all, not just the “ta-dah” at the end of the story. So in this case, as I do with preceptors in my clinic and students in my courses, I will try to be as transparent as possible, and to the best of my recall, explain the patient to you and model how I used Cycles and Segments thinking in prescribing a remedy.
This 52 year old woman presented with the chief complaint of vertigo. The first time she experienced this problem was three years before our first visit. She had a complete medical workup at that time to rule out stroke. Her EEG, EKG and echocardiogram were all normal. The onset of the vertigo coincided with her perimenopausal years. She seems hyped up, leans forward, really wants to connect, seems totally open. She is speaking quickly, the ideas are flowing rapid fire, it is as if she does not want to leave out any important detail, lots of information coming at me.
Then she had no symptoms of the vertigo for three years. About 4 months ago it began again, all of a sudden –it came on very quickly where she felt dizzy and out of touch. She felt it was difficult to get a good breath and felt as if her throat was closing up. She became anxious. She was given anti-anxiety medication from her primary care physician which did not do much and did not address her vertigo. Both seizure and cardiac disorder have been ruled out.
She feels it is related on some axis between her hormonal, neurological and mental areas. The patient reports that she was treated for depression some ten years prior. The depression did contain an anxiety component; she could not tolerate any medications each of which revved her up.
I then asked her what brought on an episode of the vertigo. She recounted two different scenarios in which she was literally crowded by people or felt crowded and overcome with emotion. She would feel she could not get enough air, felt she needed to escape. She shared an incidence of great emotional trauma which was followed by an attack of the vertigo.
At this point in the case, I began to repertorize. I had had enough time to connect with the patient, to get a feel for the flow of the case and how information was going to be shared. I already had in my mind a number of Segments, one about the vertigo, one about feeling overwhelmed. As I began choosing rubrics to populate the relevant Segments, I ask her what exactly happened at the time of the Vertigo.
She describes a splitting off, a floating away, a sort of out of body experience where she needs to get away. It is preceded by a rushing feeling in her head. Then she feels very imbalanced with a sort of expansive feeling, she feels like her head will burst, she feels like she is splitting in two. She gets into a confused sort of state, feels divided as if she will black out, though she has not. She also gets a kind of numbness at the top of her scalp and in her extremities. She does not recover fully from these episodes for days.
So here is what I have so far:
To describe the Vertigo I use the following rubrics:
Vertigo, Floating as if
Vertigo, Walking, Gliding in air…
Head, Numbness, Sensation of
Vertigo, Sudden
I called this Segment, Vertigo.
In my mind, the Vertigo lead to a broad sensation of Confusion which I represented using the following rubrics:
Mind, Delusions body is enlarged
Mind, Delusions head is enlarged
Mind, Confusion of mind, dream, as if in
Mind Delusion being double
Mind, Spaced out feeling
Mind, Confusion with Vertigo
I called this Segment, Confusion
What led my patient to these kinds of things was feeling overwhelmed by emotion and also when she felt physically overwhelmed. I put this Segment before the Vertigo Segment and called it Overwhelmed. I represented this idea with the following rubrics.
Mind, Ailments from emotions
Mind, Ailments from excitement, emotional
Mind, Sensitive to external impressions
Mind, Fear narrow places
Mind, Anxiety in a crowd
Because I am building a cycle and trying to understand her issues in a dynamic kind of way, my questions are framed in this manner. I am less interested in disparate bits of information than in understanding her issues in context. When she gets into the vertigo and the attendant confusion I need to know, what does she need to do to feel better? Is there anything that can give her some relief, or something she tries to do to alleviate the bad and strange feelings? Once I understand where I am going with the case, the questions flow in a more organic, less random fashion.
She is the type of person who will feel better if she is doing something, so she will, the best she can, try to organize things, clean the house. She can start to feel like there is something she is not doing that she is supposed to get done or that maybe she has made some mistakes. She tries to consciously pull it all together. I thought of all these kinds of things, where a patient is trying to control the situation (that is quite fair to say, out of control,) by doing. She will isolate and hunker down hyper-focusing on what she needs to get done. I will call this part of her story closing off, as she will hole up, try to get work done as best she can and keep to herself. I will use these rubrics to describe this part of her narrative:
Mind, Conscientious about trifles
Mind, Delusions , wrong, done wrong, he has
Throat, Constriction
Respiration Difficult, constriction , larynx of
Often when using Cycles and Segments we see people attempting to correct or balance a particular feeling or symptom or set of symptoms but they often overshoot the mark or need an outlet. With this patient, all that closing off ultimately creates a need for discharge.
I saw those discharges in her eager loquacity. In addition, she describes a terrific need to belch, it all bubbles up, she belches loud, hard and frequently. Indeed during our interview I had the chance to see the event, which is how you would describe it: very intense, very strong, recurrent eructations.
I used the following rubrics to represent this idea:
Mind Speech hasty
Mind, Speech loud
Stomach, Eructations- forcible
Stomach, Eructations, frequent
I called this Segment Discharges
She would feel spent and wiped out after these times of vertigo, she would try to help herself as much as she could but ultimately what she needed was someone to hold her, to put a hand on her somewhere- it didn’t matter where, it helped to ground her. Getting out of these states required that she hang out with friends, connect, laugh, spend time socially. I used the following rubrics to represent this idea:
Mind, Consolation amel.
Mind, Talking, desire to talk to someone
Mind, Held , desire to be held
Min Caressed bring, desire to be caressed
But unfortunately, she would overdo, get over-stimulated and overwhelmed by the group, all the connections and the rushing-in feeling would begin all over again leading back to the vertigo.
As I was building her Cycle I saw this very open part-connecting so much with me and as she described, with others, with emotions, with grief, that she actually disconnected—so the logical thing for me to ask was—was there any way in which she was closed or constricted? When asked that, she said that in her role as caretaker in the family and among friends, she would love it to begin, but then she would be like a social worker, running around, trying to help everyone. As she would overdo she would start to feel constricted- rule bound, having to be sure she did everything right. She also felt constricted in her creative expressions, never giving herself enough time or space to do the things she wanted to do that were expressive and creative. She would get stressed out, her symptoms, especially her GI issues would worsen, everything would come out, her words, her ideas about helping people, her belching
Her sleep is shallow, awakes often in the middle of the night. She sleeps in all positions. Her review of systems and physical generals are otherwise unremarkable.
Here is the cycle I built for her, followed by a screen shot of the rubrics used to represent the Segments. The very last shot represents all the remedies that came through six Segments. It does not mean that all of these remedies were in every rubric of a Segment, but rather that they were in at least one rubric. In this last screen, I have highlighted the remedy I chose to give her; what appears to the right in that screen are all the rubrics that particular remedy is found in.
Overall Cycle:
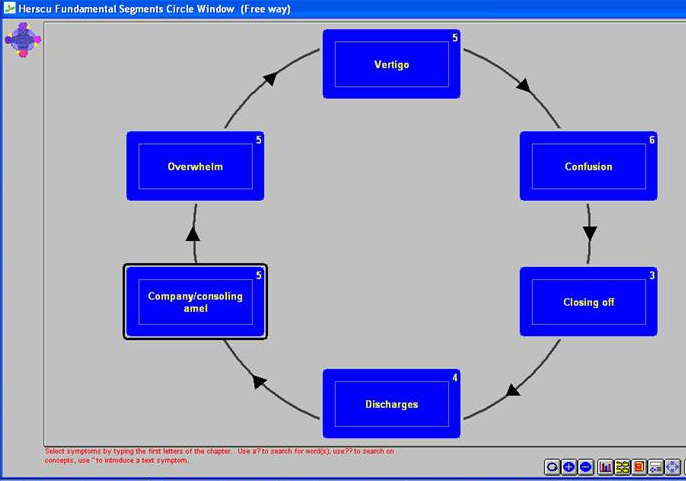
Rubrics used to represent each Segment:
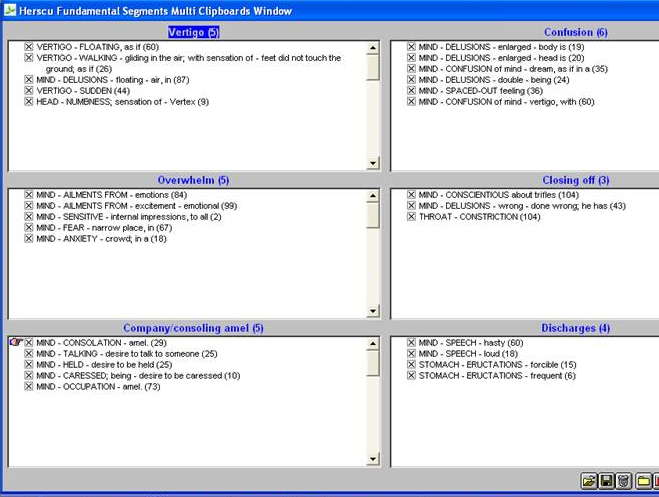
A very useful attribute of this module is that in this screen you can move rubrics to different Segments. For instance, if you wanted to put the numbness in the confusion Segment you can just highlight and drag it there. When I am taking a case, I often just grab rubrics as I am going and then sort them according to Segments a bit later, it depends on how fast information is coming at me. When we teach, sometimes we like to have the RADAR up and running and projected on a screen for all to see, then participants can see how we are thinking, which rubrics we are grabbing based on what the patient is saying as well as on what we are observing and what we are perceiving. This transparency also shows students how we make mistakes and self-correct, which anyone who has been practicing for a while does all the time and nearly unconsciously. Perhaps I see that one path I have gone down based on an assumption made, was in fact, wrong. This is one of the very useful aspects of this tool, for practitioner and student alike. Showing students how I am thinking is also useful with regard to rubric choice, how I might transfer something a patient says into repertory language, etc.
Here are the remedies that came through all six Segments:
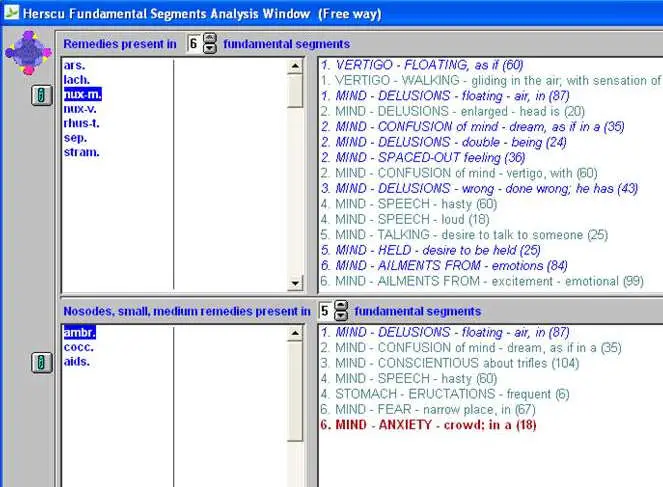
With this approach, as with any repertorization, I am not looking for one or two or even three remedies to come through. I am looking for 6-12 or so remedies. I want a list that I can say with a strong degree of confidence my patient will need and respond to one of these remedies. Then, I will go through those remedies one by one and rule them in or out, to come up with my shorter list of options.
When I do this with groups of students, we can always strike 2-3 from the list based on physical generals or a kinesthetic experience of the patient or on prior knowledge. A final decision is based on knowledge of materia medica, including an understanding of the Cycle of that remedy, my past experience and how the patient fits in with regard to the nature of the complaint.
For example, if I have a patient with a urinary tract complaint and I am trying to decide between two remedies that share a Segment or two, and one has more affinity for the urinary system, that would be one factor in my decision-making. I am also always paying attention to more specific information like physical generals and the kinds of acute illness the patient may experience.
I am looking to get the list down to 3-4 remedies by this culling process. I would then make my first, second, third and fourth choices. This way I have built a sort of scaffolding under me; should my first choice remedy not be effective, I do not have to start from a blank page. I may greatly readjust or slightly edit my repertorization on follow-up to better represent the patient, as their descriptions, my observations or my understanding of either may have evolved. Perhaps further information or diagnostic work is discovered or shared. If all is the same and I feel good about my understanding of the patient, I may go to my second choice directly.
I am able with the RADAR program, to move whole Segments if I see that the order should be different, based on how the patient explains their situation; this will not change the remedies that come through the repertorization process, but it may well influence my understanding of the patient which I compare to my understanding of the materia medica. I am also able to move individual symptoms from one Segment to another, as described above, if it seems more exacting.
I gave this patient one dose of Nux moschata 200c and asked her to return in six weeks. I thought that the remedy should help her either not have the vertigo any more or decrease the intensity and duration of episodes. I would also be looking to see her calmer, less worried and more able to enjoy her life. I shared these expectations with her and also wrote them down for myself. This helps at the time of the follow-up visit. If I am giving a specific remedy, I should know what I expect the remedy to do.
When she returned, her vertigo had abated, she felt more grounded and less spaced out. Funny thing to her was, her belching was completely alleviated. I worked with this patient over the following number of years. She eventually needed the remedy Calcarea carbonica, which she did very well with. She has occasionally come back to see me over the ensuing decade and responds well to Calcarea carbonica for most small complaints that arise. She has not had another episode of vertigo.
This manner of case taking and analysis is a holistic way of seeing the patient, and better reflects the elegant holistic philosophy which is at the heart of homeopathic medicine, where all elements of a patient’s story can be sought and represented in analysis. Repertorizing in this manner presents fewer shortcomings and more safeguards to preventing some of the vexing elements of repertorizing, where too many remedies come through, not enough remedies come through, or worse, a short list of possible remedies is arrived upon, but none seem appropriate based on prior experience or the study of materia medica. By grouping symptoms that represent the same idea into Segments and by seeing how one Segment can lead to another, I have more structure in my case taking and my ability to understand my patients is supported while my work in both case- taking and analysis is enhanced. My clinic days are more efficient; I take home only the occasional case for further study. I feel I can teach authentically what I do and can give students and colleagues a methodology which is at once internally consistent and informs every aspect of homeopathic study from how to take a case, to how to conduct and assess a proving, to the use of the repertory and the study of materia medica. For those with a lot of experience in homeopathy, that knowledge and experience can be viewed through a Cycles and Segments lens; for those newer to homeopathy, Cycles and Segments shortens the learning curve and gets you “in the ballpark” of effective remedies for patients sooner than later.
Please feel free to contact me with questions about this approach. Keep learning, keep trying, stay open and know that your efforts in learning are well worth it, for being able to help any another person in this life, even in small ways is a gift for both patient and provider.
At first, most we taught had come to us from other walks in the homeopathic world. They could take what they already knew and filter it through this philosophical lens. Sometimes there would be moments of disbelief or resistance, but mostly I would see relief. Paul and I have also taken people very new to homeopathy and some of them quite young, just starting out in this profession and showed them this way. These young people, mostly naturopathic medical school students, absorb this user-friendly, commonsense and coherent approach and can apply many of the philosophical components to other aspects of their studies, their work with patients and their lives.
*Available from www.nesh.com


