

ABSTRACT
INTRODUCTION
Psoriasis in children presents clinically similar to the adult condition. The most common clinical form of psoriasis in teenagers is plaque psoriasis. Adolescents are less likely to exhibit the inverse, palmoplantar, and guttate forms, which are typical in new-borns and young children. I want to go into detail about a case study involving plaque psoriasis and its relevance to homoeopathy.
CASE SUMMARY: Patient presented with the complaint of reddish circular eruption with scaly patches all over the head and palms, nails, ear, leg, and foot except for the face and sole for 10 years. After detailed case taking and repertorization, patient was prescribed Nux vomica 0/1 7 doses 1D/ day repeated for 7 weeks and Nux vomica 0/2 alternate hs for 2 weeks, inbetween placebo. At the last follow-up complaints of the patient were completely cured.
CONCLUSION: Homoeopathic physicians can treat a wide range of illnesses if they have the proper training and expertise. Plaque psoriasis was successfully treated with a well-chosen homoeopathic constitutional medicine, resulting in improved physical and mental health for the patient.
KEYWORD: Individualised homoeopathic medicine, Nux vomica, plaque psoriasis, repertorization.
INTRODUCTION:
The clinical picture of psoriasis in childhood resembles that of the adult disease.[1] Plaque psoriasis is the most frequent clinical type of psoriasis occurring in adolescents. [2] The inverse, palmoplantar, and guttate forms, which are frequent in infants and children, are less common in adolescents.[3]
Psoriasis is a genetically predisposed, chronic, remitting and relapsing inflammatory skin illness. Psoriasis affects 1% to 3% of the world’s youth, constituting a debilitating condition with severe social and economic consequences [4]. Skin inflammation and hyperproliferation are the hallmarks of psoriasis.
Scaly, erythematous plaques that are well-defined, affecting the extensor surfaces and the scalp, are typical features of this condition [5]. Stress, systemic medicines, sunlight, infections, and moderate trauma are all potential external and internal causes of psoriasis [6].
According to the World Health Organization, the prevalence of psoriasis is between 0.09 percent and 11.4 percent worldwide. Genetic and environmental variables are likely to have an important role in the development of the disease [7]. 90% of persons with the disease have some type of psoriasis vulgaris, which is also known as chronic stationary or plaque-like psoriasis. This is the most common form of the disease.
When elevated patches of irritated skin covered by silvery-white scaly patches are observed, it is probably the condition known as Plaque Psoriasis (PP). Plaques can be observed on the elbows, knees, scalp, and back of the neck [8]. More than one type of psoriasis affects roughly 10% of sufferers.
Pupil, inverse, nappy, guttate, oral and seborrheic-like forms [9] are some of the variations. Dermatologically, the skin is excessively thick and fast-growing in psoriasis. Pathological processes in psoriasis lead to abnormal skin cell synthesis and an excess of skin cells [10].
Genetic and environmental variables are intertwined in this illness of T cells. However, it can occur at any age, with the 20-30 year old age group having the highest prevalence. Patients can get psoriasis at any age, although the two most typical peaks occur in their early third decade and their mid-fifth decade [11].
Psoriasis is mainly diagnosed by looking at the skin. Plaques, papules, or patches of scaly, erythematous skin characteristic of psoriasis may be uncomfortable and itchy. The diagnosis is frequently made without the need for any specific blood testing or diagnostic procedures [12,13]. Dermatological testing may be necessary to rule out other conditions and confirm the diagnosis if the clinical diagnosis is in doubt.
Epidermal protrusions that interdigitate with the dermis can be seen on microscopy from a biopsy skin sample. Physical, emotional, and social problems are enormously exacerbated by psoriasis. In general, people’s well-being is frequently seriously harmed as a result. For both people and society, mental well-being has a substantial cost, such as increased rates of depression.
For those who have psoriasis and their families, social exclusion, prejudice and stigma can have a catastrophic psychological impact[3]. Psoriasis is currently thought to be an inherited autoimmune disease that can be controlled rather than cured with current medications. Smoking cessation, the use of topical treatments, phototherapy or photo-chemotherapy, and systemic therapy are all part of the treatment plan. [14].
Dr. Samuel Hahnemann wrote in the 186th aphorism of the Organon of Medicine. about those so-called maladies that were caused a short time ago, simply by an external lesion, and still appear to justify the designation of local sickness at first glance.
The treatment of such disorders is limited to surgery; however, this is correct only in so far as the damaged portions require mechanical assistance, in order to eliminate the external obstacles to the cure, which can only be expected to occur through the agency of the vital force…etc. However, when the whole living organism demands active dynamic aid to put it in a position to do the process of healing, as it always does, the services of the dynamic are required. [15]
Similar research was undertaken by Annu Kanwar on the role of individualised homoeopathic medicine Lycopodium in plaque psoriasis, which the patient had suffered from for three years. One year later, after homoeopathic treatment with Lycopodium 200 C and 1M, the patient showed improvement.[16]
Homoeopathy acts better as a constitutional remedy in cases of psoriasis when we consider each case in a holistic individual manner and with the totality of symptoms. One such case, which improved satisfactorily by homoeopathic treatment, is presented.
CASE PRESENTATION:
The patient was a 17 year old male, Hindu by religion, studying 11th standard who presented with the complaint of reddish circular eruptions with scaly patches with occasional itching all over the body except face, trunk and soles for the last 10 years.
CASE REPORT:
The patient complained of a reddish eruption. It first developed on the scalp (Figure 1) and then spread to other parts of the body, except the face, trunk, and soles. The eruptions were primarily found on the head, the exterior aspect of the lower limbs, and the foot dorsum.
The patient had extreme itching in eruptions, followed by intense scratching and bloody discharge. Scaling is seen on the scalp, ears, palms, legs, and dorsum of the foot. By scratching, complaints were alleviated, and there were bleeds after scratching and washing. No history of blisters, fever, arthralgia, no substantial family history.
PAST HISTORY:
No relevant past medical history. Patient received allopathic treatment for the presenting problems, but no changes were seen.
LIFE SPACE INVESTIGATION:
The patient was born into a middle-class household and reached age-appropriate developmental milestones normally. He was quite calm and had good relationships with his family and friends. He had a few school buddies, and he sometimes felt horrible about associating with them as he was experiencing skin problems.
He would get angry whenever anybody mentioned his complaint. If his sister discussed his complaints, he became furious and beat her. Occasionally, he flung objects during anger. He was shy person who does not interact readily with others. He uses gestures while speaking and provides single-word responses. Aside from math, he was a good student.
PERSONAL HISTORY:
- PHYSICAL GENERAL: appetite- good (3 times/day), thirst-normal (2.5L/day), sleep-good (8-9 hours/day), urine-normal (5-6 times/day), stool-regular (1 time/day, normal consistency), sweat-more on head, thermal-chilly patient.
- MENTAL GENERAL: Reserved+++, Timid+++, Anger violent+++, Monosyllabic++, makes gestures++.
PHYSICAL EXAMINATION:
- GENERAL EXAMINATION: lean appearance, moderate-built and nourished, no signs of pallor, cyanosis, clubbing, edema, lymphadenopathy, Vitals stable
- SYSTEMIC EXAMINATION: reddish circular eruption with scaly margins all over head, exterior leg and dorsum of foot. well defined border of the lesion, width of lesion >2 cm, scaling of silvery scales of the head and ear onycholysis in nails seen. no signs of clubbing, nail pitting, On palpation- Hard crust with raised flat eruptions, auspitz sign positive.
LAB INVESTIGATION:
BLOOD ROUTINE: Hb-13.9mg/dl, total WBC count- 8.7 K/ul, differential count neutrophil-59%, lymphocytes-39%, eosinophil-02%, ESR 30MTS-6mm, ESR 60MTS-12mm.
DIAGNOSIS OF THE CASE:
After detailed case taking with examination and investigatory finding the patient was diagnosed with plaque psoriasis.
MIASMATIC DIAGNOSIS: Fundamental miasm: PSORA, Dominant miasm: SYCOSIS
CLINICAL COURSE: Considered symptoms for the constitution:
- Reserved
- Timid
- Anger violent
- Gestures making
- Scaly Eruptions on head
- Dry scaly psoriatic patches
- Itching < perspiration. > scratching, bleeding after
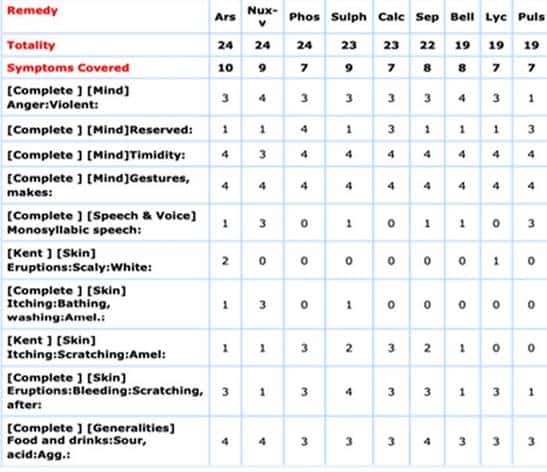
REPERTORISATION: Was done using Zomeo 3.0 (Hompath 11 version).[17]
Fig-1: Repertorial Chart
INTERVENTION: 1st prescription was on 19th of December 2021
Rx Nux vomica 0/1, 0/2, 0/3 1D per day was given as per the homoeopathic principle.
ADVICE: To maintain proper skin hygiene and to have moist skin and avoid dust exposure.
FOLLOW UP CRITERIA:
- Itching of the psoriatic lesions
- Scaling of psoriatic lesions,
- Psoriatic eruptions
- Generals
| DATE | SYMPTOM CHNAGES | PRESCRIPTION- INTERVENTION |
| 08/01/2022 | Itching of the psoriatic lesions – persist as same. Scaling of psoriatic lesions – persist as same. Psoriatic eruptions – persist as same. Generals – good | Rx 1.Nux vomica 0/1/7D- HS 2. Sac lac 7D (1D-Alternate HS) 3.B.Pills 3xtds |
| 15/01/2022 | Itching of the psoriatic lesions – reduced than before. Scaling of psoriatic lesions – reduced than before Psoriatic eruptions – reduced than before Generals – good | Rx 1.Nux vomica 0/2/7D- HS 2. Sac lac 7D (1D-Alternate HS) 3.B.Pills 3xtds |
| 12/02/2022 | Itching of the psoriatic lesions – better Scaling of psoriatic lesions – better Psoriatic eruptions – slight change than before. Generals – good | Rx 1.Nux vomica 0/3/14D- HS 2. Sac lac 7D (1D-Alternate HS) 3.B.Pills 3xtds |
| 12/03/2022 | Itching of the psoriatic lesions – absence of symptoms Scaling of psoriatic lesions – Better than before Psoriatic eruptions – Better than before Generals – good | Rx 1.Nux vomica 0/4/14D- HS 2. Sac lac 7D (1D-Alternate HS) 3.B.Pills 3xtds |
| 09/04/2022 | Itching of the psoriatic lesions – Complete cure no itching Scaling of psoriatic lesions – Complete cure no scaling of lesion Psoriatic eruptions – complete cure eruptions dried up Generals – good
|
Rx 1.Nux vomica 0/5/14D- HS 2. Sac lac 7D (1D-Alternate HS) 3.B.Pills 3xtds |
| 14/05/2022 | No itching and scaling, no recurrence of symptoms
Generals – Good |
Rx 1.Sac lac 14D 1D/Day 2.B.Pills 3xtds. 3.B.Disc 1xbd |
RESULTS: Gradually, the patient improved symptomatically after the prescription of the homoeopathic medicine Nux vomica 0/1- 7D daily HS for 1 week repeated for 7 weeks followed by Nux vomica 0/2,0/3,0/4,0/5. In- between placebos were prescribed.
Within a few weeks marked improvement was seen in the complaint of the patient (Fig-3). In the last follow-up, complaints of the patient were completely cured. There were significant changes in all the symptoms and silvery scaling from the psoriatic lesions- which resolved completely within 8 weeks (Fig-4) (total treatment period 8th of January 2022-22th of May 2022)
The patient showed marked improvement in symptoms when a dose of Nux-vomica 0/1,0/2,0/3,0/4,0/5 was given as constitutional medicine repeated for 3 months, inbetween placebo was prescribed. At the last follow-up, complaints of the patient were completely cured. Total treatment period was 90 days from 8th of January 2022 -22th of May 2022. After the first administration of the Nux-vomica 0/1,0/2,0/3,0/4,0/5.
TREATMENT FIGURES
Fig2: Before Treatment.

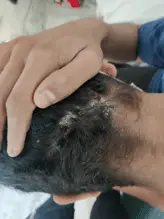


Fig-3: During Treatment




Fig-4: After Treatment




TABLE 2: ASSESSEMENT BY MODIFIED NARANJO CRITERIA SCORE. [18]
| ITEM
|
YES | NO | NOT SURE |
| Was there an improvement in the main symptom or condition, for which the homoeopathic medicine was prescribed? | +2 | ||
| Did the clinical improvement occur within a plausible time frame relative to the drug intake? | +2 | ||
| Was there an initial aggravation of symptom? (Need to define in glossary) Did the effect encompass more than the main symptom or condition, i.e., were other symptoms ultimately improved or changed? |
0 | ||
| Did overall well-being improve? (Suggest using validated scale) Direction of cure: Did some symptoms improve in the opposite order of the development of symptoms of the disease? | +2 | ||
| Did the clinical improvement occur within a plausible time frame relative to the drug intake? | 0 | ||
| Was there an initial aggravation of symptom? (Need to define in glossary) Did the effect encompass more than the main symptom or condition, i.e., were other symptoms ultimately improved or changed? |
0 | ||
| Direction of cure: Did at least two of the following aspects apply to the order of improvement of symptoms: 1.From organs of more importance to those of less importance 2. From deeper to more superficial aspects of the individual 3. From the top downwards |
+1 | ||
| Did ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | +1 | ||
| Are there alternate causes (other than the medicine) that – with a high probability – could have caused the improvement? (Consider known course of disease, other forms of treatment and other clinically relevant interventions) | 0 | ||
| Was the health improvement confirmed by any objective evidence? (e.g., laboratory test, clinical observation | +2 | ||
| Did repeat dosing, if conducted, create similar clinical improvement? | 0 | ||
| TOTAL SCORE= 10 |
DISCUSSION:
Handling such cases needs proper investigation of the patient homoeopathically by knowledgeable physicians. Such cases are generally treated by conventional medicine which comes with side effects. However, homeopathy can treat them in a rapid and gentle manner.[15].
This study suggests that with proper homoeopathic investigation of the patient constitutional treatment leads a better outcome physically and emotionally. This patient suffered for 10 years during his prior treatment with no alleviation of his complaint.
Similar research was undertaken by Annu Kanwar on the effects of homoeopathic Lycopodium 200 C and 1M on plaque psoriasis, which the patient had been dealing with for three years. The patient experienced relief after one year of treatment. Thus, in this study, individualised homoeopathic medicine Nux-Vomica in 50 millesimal potencies showed noticeable improvement in the first month. This study therefore recommends utilising individualised homoeopathic medicine in 50 millesimal potencies to speed up the patient’s recovery.[19].
A study was conducted by Dr. Mayuri Mahale and Dr. Suvarna Patil -Homoeopathic Management of Psoriasis: A case study evidences the role of the homoeopathic medicine Nux vomica in treating the psoriasis. [20].
A study done by Dr. Bhaskar Sarkar and Dr. Maurya Manjurani Sheopal – Psoriasis improved homoeopathically: A case report suggested that one of the most effective treatments for chronic skin conditions is Sulphur, which was first administered in this instance of psoriasis, followed by Nitric acid, the second most effective treatment, following repertorisation and keeping the totality picture in mind.
In 18 months, the psoriatic skin condition and other bodily issues that had been present for 27 years disappeared. Comparing with this study our patient’s improvement was seen within a month after administering a single constitutional remedy, Nux vomica in fifty millesimal potency. [21].
A prospective, multicenter observational study found that homoeopathic treatment considerably reduced the severity of psoriasis and related disorders, as well as improving quality of life, while lowering the usage of conventional medicine and health services. [22].
Homeopathy can often provide a gentle, curative therapy for this disorder.[23]. Homeopathy treats the individual patient rather than the named disease and with no side effects. Master Sammuel Hahnemann discusses local maladies and the scope of homoeopathic constitutional medicine Aphorisms 185-203 in Organon of Medicine.[15]
This type of study may help patients to accept homoeopathy and get benefit from the illnesses where other medical systems have a limited role.
CONCLUSION:
This case emphasises the importance of symptom similarity with individualization of medication, demonstrating the efficacy of homoeopathic medicine in the treatment of plaque psoriasis. More evidence-based clinical trials must be done to further demonstrate the efficacy of homoeopathic medicine in such challenging cases.
FUND: financial support and sponsorship none.
PARENTS CONSENT: Obtained
CONFLICT OF INTEREST: None declared.
Address for acknowledgement: Sarada Krishna Homoeopathic Medical College, Kulasekharam,Kanyakumari District, Tamilnadu-629-161
REFERENCES:
- Raychaudhuri SP, Gross J.A comparative study of pediatric onset psoriasis with adult onset psoriasis. Pediatr Dermatol. 2000;17(3):174–178. doi: 10.1046/j.1525-1470.2000.01746.x [PubMed] [CrossRef] [Google Scholar]
- Ferrándiz C, Pujol RM, García-Patos V, Bordas X, Smandía JA.Psoriasis of early and late onset: a clinical and epidemiologic study from Spain. J Am Acad Dermatol. 2002;46(6):867–873. doi: 10.1067/mjd.2002.120470 [PubMed] [CrossRef] [Google Scholar]
- Bonigen J, Phan A, Hadj-Rabia S, et al.Impact de l’âge et du sexe sur les aspects cliniques et épidémiologiques du psoriasis de l’enfant. Données d’une étude transversale, multicentrique française. Ann Dermatol Venereol. 2016;143(5):354–363. doi: 10.1016/j.annder.2016.02.006 [PubMed] [CrossRef] [Google Scholar]
- Zhu JF, Kaminski MJ, Pulitzer DR, Hu J, Thomas HF. Psoriasis: pathophysiology and oral manifestations. Oral diseases. 1996 Jun;2(2):135-44. [PubMed] [CrossRef][Google Scholar]
- Walker BR, Colledge NR, Ralston S, Penman ID, Britton R, editors. Davidson’s principles and practice of medicine. 22nd edition. Edinburgh; New York: Churchill Livingstone/ Elsevier 2014, 1286-1289p [PubMed] [CrossRef][Google Scholar]
- World Health Organization. Global diffusion of eHealth: making universal health coverage achievable: report of the third global survey on eHealth. World Health Organization; 2017 Mar 27.
- Krueger JG, Ferris LK, Menter A, Wagner F, White A, Visvanathan S, Lalovic B, Aslanyan S, Wang EE, Hall D, Solinger A. Anti–IL-23A mAb BI 655066 for treatment of moderate-to-severe psoriasis: Safety, efficacy, pharmacokinetics, and biomarker results of a single-rising-dose, randomized, double-blind, placebo-controlled trial. Journal of Allergy and Clinical Immunology. 2015 Jul 1;136(1):116-24.
- Palfreeman AC, McNamee KE, McCann FE. New developments in the management of psoriasis and psoriatic arthritis: a focus on apremilast. Drug design, development and therapy. 2013;7:201.
- James W, Berger T, Elston DA, Andrews GC. Diseases of the Skin. Clinical Dermatology. 2005;10:1-1.
- Ouyang W. Distinct roles of IL-22 in human psoriasis and inflammatory bowel disease. Cytokine & growth factor reviews. 2010 Dec 1;21(6):435-41.
- Mittal A. Illustrated synopsis of dermatology and sexually transmitted diseases. Indian Journal of Dermatology, Venereology, and Leprology. 2016 Jul 1;82(4):474-.
- Tan IJ, Peeva E, Zandman-Goddard G. Hormonal modulation of the immune system—a spotlight on the role of progestogens. Autoimmunity reviews. 2015 Jun 1;14(6):536-42.
- Johnson MA, Armstrong AW. Clinical and histologic diagnostic guidelines for psoriasis: a critical review. Clinical reviews in allergy & immunology. 2013 Apr;44(2):166-72.
- Homoeopathy in psoriasis vulgaris: A case report. ABC of dermatology- 6 th edition-London, UK 2014, 18. Nisha CN.
- Samuel H. Organon of the medicine, English translation of 6th & 5th German edition by William Boericke & RE Dudgeon, corrected, retranslated & redacted by Dr. Mahendra Singh & Dr Subhas Singh. 2nd ed. Homoeopathic publications, Kolkata. 2015:17-225.
- Kanwar A, Ram H, Kumar N, Bagdi N. Plaque Psoriasis Successfully Treated with an Individualised Homoeopathic Medicine Lycopodium: A Case Report. Homœopathic Links. 2020 Sep 8.
- Homeopathy Software | Repertory – Hompath Zomeo https://hompath.com › zomeo
- Belhekar MN, Taur SR, Munshi RP. A study of agreement between the Naranjo algorithm and WHO-UMC criteria for causality assessment of adverse drug reactions. Indian journal of pharmacology. 2014 Jan;46(1):117.
- Wiesenauer M, Lüdtke R. Mahonia aquifolium in patients with Psoriasis vulgaris—an intraindividual study. Phytomedicine. 1996 Nov 1;3(3):231-5.
- Mahale M, Patil S. Homoeopathic management of psoriasis: A case study.
- Sarkar B, Sheopal MM. Psoriasis improved homoeopathically: A case report.
- Witt CM, Lüdtke R, Willich SN. Homeopathic treatment of patients with psoriasis – a prospective observational study with 2 years follow-up- Journal compilation-European Academy of Dermatology and Venereology – JEADV 2009;23:538-543.
- Boericke W. Pocket Manual of Homoeopathic Materia Medica & Repertory: Comprising of the Characteristic and Guiding Symptoms of All Remedies (clinical and Pahtogenetic [sic]) Including Indian Drugs. B. Jain publishers; 2002.


I don’t understand what potencies of Nux vomica were used, i.e. “0/1- 7D daily HS for 1 week repeated for 7 weeks followed by Nux vomica 0/2,0/3,0/4,0/5.” If these were LM potencies, why weren’t they described as LM1, or LM2, etc? Other than not being able to understand the potencies prescribed, I thought the article was quite helpful.
Hi Linda! 0/1 means LM1. 7D is the way Europeans say 7X. HS is an abbreviation I’ve never heard before. However, this looks like another “protocol” to me. Whatever happened to Hahnemann’s admonition that a striking improvement precludes all further dosing for as long as the improvement lasts, and if a patient aggravates, stop dosing. Once you establish a protocol, there’s no room for Hahnemann’s aphorisms anymore. I have no idea what 0/1-7D daily means.
OK, Linda,
“Nux vomica 0/1 7 doses 1D/ day repeated for 7 weeks”
probably means Nux v. LM1, 7 doses, one dose a day, for 7 weeks.” Then,
“Nux vomica 0/2 alternate hs for 2 weeks”
probably means, Nux v. LM2 on alternate days for 2 weeks, but I’m not sure of that! It’s not so much “HS” as it is “H”, with the “S” making it plural. Still, not sure what H stands for.
Me again.
“Rx Nux vomica 0/1, 0/2, 0/3 1D per day”
I’m thinking this means: LM1, LM2, LM3, one dose per day”
I’m stumped regarding the “HS” abbreviation. Frankly, I’m not sure how they came up with Nux v. since Arsenicum scored higher. Yes, Nux v. is a violent remedy; not so much thought of as “timid” though.
Thank you…
First or second alone will not decide the remedy mam/sir after repertorization i had appeal with materia medica where it exactly matches with the patient from mind n generals so i have given nux instead of ars…
You’re right, coming in first or second in a repertorization doesn’t mean you’re obligated to pick that remedy. It is important to check with the Materia Medica first for confirmation.