

Reprinted with permission from the Indian Journal of Applied Homoeopathy where it first appeared. https://www.jimshomeocollege.com/ijah-publications/
Background of Study:
This study was carried out with a cross-functional team of doctors including pediatrician and homeopath in a rural hospital setting in India from 1997-99. There were limited lab investigations available at our disposal and major clinical decision making was based on bedside clinical examination findings. Clinical judgement hence, played a major role in determining therapeutic strategy. Software “Organon 96” was used for systematic documentation and analysis of homoeopathic cases right fromsymptom recording, symptom analysis, homoeopathic totality, Repertorization, potency selection and second prescription, which improved the precision of homoeopathic management.In order to understand the intricacies of homoeopathic management based mainly on concept Susceptibility and Miasm it is imperative to revise the clinical information of AGN.
Introduction:
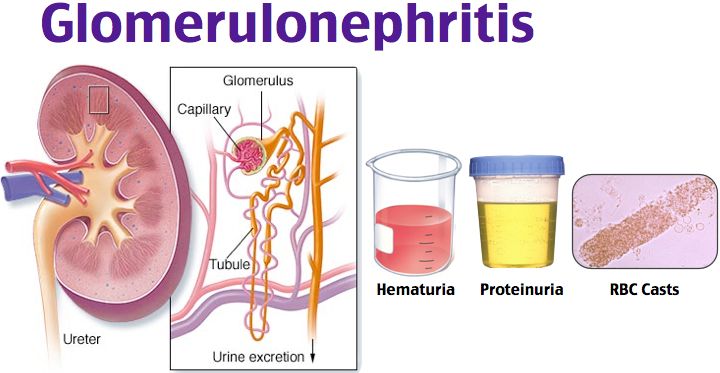
The term Glomerulonephritis signifies glomerular inflammation in which, there is an immunologically mediated injury to the glomeruli. Nephritic syndrome resultant of glomerulonephritis is characterized by the sudden onset of gross hematuria, edema, hypertension, and renal insufficiency. Acute post streptococcal glomerulonephritis is one of the most common glomerular causes of gross hematuria in children, surpassed only by IgA nephropathy.
Etiology:
- Infectious diseases: Post streptococcal Glomerulonephritis follows infection of the throat or skin by certain “nephritogenic” strains of group A β-hemolytic streptococci), infective endocarditis, syphilis, mumps, measles, hepatitis B, infectious mononucleosis, Epstein Barr virus infection, malaria, HIV-associated nephropathy.
- Multisystem diseases: SLE, Good pasture’s syndrome, Henoch-Scholein Purpura, microscopic polyangiitis, Wegener’s granulomatosis, sickle cell nephropathy.
- Primary glomerular diseases: Diffuse proliferative Glomerulonephritis, IgA nephropathy, Mesangio-capillary Glomerulonephritis, Crescentic Glomerulonephritis, membranous Glomerulonephritis, focal segmental glomerulosclerosis.
- Miscellaneous: malignancy, eclampsia, penicillamine.
Pathogenesis:
Normally, the immune complexes formed in the body are removed by the host’s Reticuloendothelial System (RE). Impaired ability on the part of the host to clear immune complexes may result in their deposition in the glomerular capillary walls.
Two chief pathogenic mechanisms are recognized: Deposition of antigen antibody complexes (immune complexes) in the glomeruli resulting in glomerular disease; and deposition of an antibody in theglomerular basement membrane which then reacts with an antigen in the basement membrane causing glomerulonephritis.
The mechanism of post streptococcal acute diffuse proliferative glomerulonephritis is immune mediated where granular deposits of IgG and C3 (“humps”) occurs on the external (sub epithelial) side of the basement glomerular membrane. The antigen involved in the immune complex formation may be exogenous (eg. Bacteria such as streptococci as in post streptococcal Glomerulonephritis) or endogenous (eg. antibodies to host DNA in patients with SLE).The immune complexes and antibodies against a glomerular antigen, trigger injury by the following mechanisms: Complement activation; Fibrin deposition; Platelet aggregation; Release of cytokines and free oxygen radicals.
Discussion:
From a homoeopathic perspective it is important to note that AGN is the result of an “Aberrant Immune (RE) System”, thus the seat of illness is RE system and Kidney GBM is the target tissue. If an individual’s RE system has the ability to clear immune complexes the proneness of an individual to fall prey to AGN reduces. The above discussion helps reflect on pathogenic vulnerability of an individual which is a basisfor understanding susceptibility and Miasm.
Pathology:
Immune-fluorescence microscopy reveals lumpy-bumpy deposits of immunoglobulin and complement on the glomerular basement membrane (GBM). On electron microscopy, electron-dense deposits, or “humps,” (deposits of immunoglobulin and complement) are observed on the epithelial side of the GBM.
The kidneys appear symmetrically enlarged. All glomeruli appear enlarged and relatively bloodless and show diffuse mesangial cell proliferation. Increase in mesangial matrix Polymorh-nuclear leukocytes are common in glomeruli during the early stage of the disease. Crescents and interstitial inflammation may be seen in severe cases.
Discussion:
The pathological changes depicted above indicate acute inflammatory changes due to fault in the immune system of an individual and not due to infection directly. Thus, from a Hahnemannian disease classification perspective one can safely conclude that, AGN is not only “acute” but also “miasmatic in nature” due to its deeper immune system aberrances. The understanding of classification helps the clinician think in terms of posology and homeopathic remedy sequence strategy i.e. acute followed by chronic etc. to prevent relapses.
The prominent microscopic feature is a-vascularity and proliferation of target tissue i.e. membrane and mesangial cells. Mesangial cells, support the basement membrane to increase or decrease its surface area through their contractile action, thus impacting the filtrates i.e. proteins, RBC and water. From a homoeopathic perspective it is important to know that basement membrane, connective tissue and endothelium lining is targeted by the immune complexes causing deprivation of blood to tissue andswelling. These pathogenic features indicate predominance of Syco-Tubercular miasmatic activity as the central foundation of AGN though the miasmatic activity ranges from psora to syphilitic in this given disease.
Clinical features:
- Common symptoms hematuria, edema, hypertension, proteinuria and oliguria.
- Associated complaints are malaise, lethargy, abdominal or flank pain and fever.
- Occurrence of complications depend on the severity of renal involvement, ranging from asymptomatic microscopic hematuria with normal renal function to acute renal failure.
- Encephalopathy and/or heart failure owing to hypertension or hypervolemia thou rare, are distant possibilities.
- Edema typically results from salt and water retention; nephrotic syndrome may develop in 10– 20% of cases; acute subglottic edema and airway compromise have been reported.
- Usually the pace of symptom appearance is fast, once they appear they persists for 4 to 6 weeks in spite of conventional treatment.
- Prognosis: acute phase generally resolves within 6–8 wk. Although urinary protein excretion and hypertension usually normalize by 4–6 wk. after onset, persistent microscopic hematuria may persist for 1–2 yr. after the initial presentation.
Discussion:
Clinico- pathological correlations make it quite evident that, there is an array of disease expression ranging from mild to severe life- threatening complications. Pace- wise it is swift to appear but slow to disappear over 4 to 6 weeks.
There are few general symptoms in this cluster which are usual and common with many inflammatory diseases. Particular Symptoms related to kidney in this cluster do not produce pain hence, one should not expect too many characteristic symptoms as; sensations or modalities. Thus, the expression of susceptibility in terms of pain sensitivity and PQRS characteristics is expected to be frail and unexpressive.
To complicate the matters AGN has a multi-systemic involvement as resultant of accelerated hypertension includes, CVS and Brain. Due to this peculiar nature of illness apart from; mental and physical general attributes of the patients, variants of pace of the disease and symptom evolution patterns should be our guiding blocks for individualization.
Laboratory Diagnosis:
Urine analysis RBCs, RBC casts, proteinuria and poly-morph-nuclear leukocytes.
Blood smear Decreased C3 level, normochromic anemia, ASO elevated
Renal Biopsy considered during renal failure, nephrotic syndrome and no streptococcal infection
Differential diagnosis:
Summary of Primary Renal Diseases That Manifest as Acute Glomerulonephritis
| DISEASES | Post-streptococcal | IgA | Good pasture | Rapidly Progressive | ||
| glomerulonephritis | nephropathy | syndrome | glomerulonephritis | |||
| Age and sex | All ages, mean 7 yr | 10–35 yr | 15–30 yr | Adults | ||
| Sex | 2 : 1 male | 2 : 1 male | 6 : 1 male | 2 : 1 male | ||
| Acute nephritic | 90% | 50% | 90% | 90% | ||
| syndrome | ||||||
| Asymptomatic | Occasionally | 50% | Rare | Rare | ||
| hematuria | ||||||
| Nephrotic syndrome | 10–20% | Rare | Rare | 10–20% | ||
| Hypertension | 70% | 30–50% | Rare | 25% | ||
| Acute renal failure | 50% (transient) | Very rare | 50% | 60% | ||
| Other | Latent period of 1–3 | Follows viral | IDA,Pulmonary | None | ||
| wk | syndromes | hemorrhage | ||||
| Laboratory findings | ↑ ASO titers, ↓C3- | ↑ Serum IgA, | Positive anti- | Positive ANCA in | ||
| C9, Positive | IgA in dermal | GBM antibody | some | |||
| streptozyme | capillaries | |||||
| Light microscopy | Diffuse proliferation | Focal | Focal –diffuse | Crescentic GN | ||
| proliferation | with crescents | |||||
| Immunofluorescence | Granular IgG, C3 | Diffuse | Linear IgG, C3 | No immune deposits | ||
| mesangial IgA | ||||||
| Electron microscopy | Subepithelial humps | Mesangial | No deposits | No deposits | ||
| deposits | ||||||
| Prognosis | 95% resolve | Slow | 75% stabilize or | 75% stabilize or | ||
| spontaneously, 5% | progression in | improve if | improve if treated | |||
| RPGN /slow progress | 25–50% | treated early | early | |||
Complications:
Acute complications of this disease result from hypertension and acute renal dysfunction. Hypertension is seen in 60% of patients and may be associated with hypertensive encephalopathy in 10% of cases. Other potential complications include heart failure, hyperkalemia, hyperphosphatemia, hypocalcemia, acidosis, seizures, and uremia.
Prevention:
Family members of patients with acute glomerulonephritis should be cultured for group A β-hemolytic streptococci and treated if culture positive.
Management:
Treating the acute effects of renal insufficiency and hypertension and Sodium restriction are key to preventing complications.
Prognosis:
Complete recovery occurs in more than 95% of children with acute post streptococcal glomerulonephritis. Mortality in the acute stage is known but, can be avoided by appropriate management of acute renal failure, cardiac failure, and hypertension.
Homoeopathic approach in cases of AGN
After having dealt with the clinical study of acute glomerulonephritis and its homoeopathic correlations, the note that follows will help us understand the basis of therapeutic aspects of AGN. The approach is based on phenomenon of miasm and susceptibility. Some of the salient features are as follows:
Classification:
Acute glomerulonephritis from Hahnemannian disease classification is an acute miasmatic disease yet, has a potential to become chronic in the form of Nephrotic syndrome. Hence, managing the acute and preventing relapse should be the goal of homoeopathic treatment.
Homoeopathic Correlation of Pathology and Miasm.
As in most cases, AGN is a sequelae of infection which, migrates from the primary seat; skin and throat to kidneys. A consequence of Infection is metastasized in kidneys via immune complexes. Thusa sequence of events starts as an aberrant immune reaction which is fast paced with sudden onset to begin with.
Pathologically, post infection, immune complexes with complement deposits on GBM causing sustained inflammation in Kidneys. This leads to hypertension, hematuria edema and metabolic depletion. There is a cardiac overdrive, systemic congestion, cerebral congestion, and ascites as part of its pathogenesis. More dreaded are ARF, LVF and encephalopathy as life threatening complications.
From the above clinic-pathological correlations it is evident that AGN exhibits a range of miasmatic activity from psora to syphilitic. Psoric activity is simple proteinuria with a rapid pace and hypersensitive reactions, with quick responses of the body, which reverse quickly. If the pace is slow, with gradual evolution of pathogenesis, a dull deviant mechanism, with predominant symptom of edema, it is more likely to be the SycoticMiasm in action.
Many cases depict tubercular Miasm, understandably so, as the primary system getting involved is the Reticulo-endothelial with the target organ as kidney ( RE). Acutely generated Immune Complex Deposits cause sustained inflammation with bleeding, cardiac overdrive organ failures and multi-systemiclife-threatening complications. There is fast pace, multisystem involvement and certain unpredictability of complications inherently inbuilt in AGN, all classic hallmarks of tubercular diathesis.
Though AGN is structurally reversible pathogenesis, it may turn into irreversible pathology at the drop of a hat. When the pace is fast with complications of persistent hypertension as: encephalopathy or left ventricular failure and ARF, then it’s anybody’s guess that the case is approaching the Syphilitic miasmatic zone.
Quantifying Susceptibility based on Pattern of Disease Evolution:
This understanding is based only on evolution of disease phenomenon. Each disease phenomenon thoughit has a generic pattern is also highly individualistic. When, individual characteristics of involved organ or system (kidney) are not in abundance as in AGN, the pace of disease, pattern of evolution and progress is often the savior. The trio of pace, pathology and characteristic help decide the homeopathic strategy to manage these complex expressions of AGN.
Based on the above conceptual understanding of susceptibility and miasm a case series study was conducted in 1997. The Table illustrates the essence of the ten sample cases, which includes: symptoms, pace, duration, associated complaints, possible etiology:
Clinical Data of Sample Cases:
| Clinical Data Table of Sample Cases | |||||||||||||||||||||||
| Case # | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||||||||||||
| Age in Years | 7 | 17 | 5 | 17 | 11 | 5 | 11 | 8 | 12 | 10 | |||||||||||||
| Gender | F | F | M | M | M | F | F | F | F | M | |||||||||||||
| (Male/Female) | |||||||||||||||||||||||
| Onset | S | G | G | G | S | S | S | S | G | S | |||||||||||||
| (Sudden/Gradual) | |||||||||||||||||||||||
| Duration in Days | 4 | 15 | 10 | 10 | 7 | 6 | 7 | 3 | 2 | 2 | |||||||||||||
| Edema (Grade I to 4) | 2 | 2 | 2 | 4 | 3 | 2 | 2 | 1 | 2 | 3 | |||||||||||||
| Proteinuria (1+ to 4 | 3 | 2 | 4 | 3 | 3 | 4 | 3 | 1 | 3 | 3 | |||||||||||||
| +) | |||||||||||||||||||||||
| Hematuria | P | P | P | P | P | P | P | P | P | P | |||||||||||||
| (Present/Absent) | |||||||||||||||||||||||
| Hypertension ( | 130/ | 150/8 | 140/9 | 150/ | 170/9 | 130/80 | 170/12 | 160/ | 140/ | 130 | |||||||||||||
| Present/Absent) | 80 | 0 | 0 | 90 | 0 | 0 | 100 | 80 | /80 | ||||||||||||||
| Oliguria ( | P | P | A | A | A | A | A | A | P | A | |||||||||||||
| Present/Absent) | |||||||||||||||||||||||
| Complications | Ascite | Hyperte | LVF | Asci | |||||||||||||||||||
| s | nsive | tes | |||||||||||||||||||||
| Headac | |||||||||||||||||||||||
| he | |||||||||||||||||||||||
| Nature of | Colic | Allergi | Bronc | URTI | Head | URTI | Colitis | URTI | |||||||||||||||
| Associated | & | c | hitis | ache | /Pyoder | Tenesm | |||||||||||||||||
| Complaints | Enur | Derm | ma& | us and | |||||||||||||||||||
| esis | atitis | CSOM | LMS | ||||||||||||||||||||
| Associated | Chro | Chroni | Acute | Chr | Chron | Acute/C | Acute | Chro | |||||||||||||||
| Complaints( Acute | nic | c | onic | ic | hronic | nic | |||||||||||||||||
| or Chronic) | |||||||||||||||||||||||
| History of Throat | # | ||||||||||||||||||||||
| Infection | |||||||||||||||||||||||
| History of Throat | # | ||||||||||||||||||||||
| Skin Infection | |||||||||||||||||||||||
CASE 1
A 7 year old girl came with complaints of proteinuria3+, edema, hematuria, blood pressure of 130/80 and oliguria. Complaints started all of a sudden after she had an episode of fever, which was precipitated after her friend sitting next to her in class was scolded by the teacher. Child received allopathic treatment initially but there was no improvement. She developed all the complaints after 4 days of the incident. She had a shocked and stunned look on her face. Associated complaints were colic and nocturnal enuresis. There was a history of throat infection in the recent past. Detailed history revealed child was fearful in nature, hot thermally and had craving for sweets.
Totality:
- A/F Fright and shock
- Suppression
- Fearful
- Hot pt.
- Cr –sweet
Discussion:
First notable observation is, no characteristics at renal system level except, a clear cause and effect. Cause and effect couplet demonstrates the vulnerability of the child to the harshness of teacher, her hypersensitivity and fear. Child’s individual system responded to reprimand with emotional shock and fright, indicating high sensitivity and vulnerability to rough behavior.
To begin with, Child was shocked and stunned, could not express her emotions. Responded with fever which was suppressed with allopathic treatment, yet the disease continued progressing. With no emotional expression finallythe disease localized in GBM of kidneys.
Childs cravings for sweets and hot patient, clinched the remedy opium. Opium 200 single dose wasprescribed, as susceptibility exhibited a good reaction. Totality was formed with help of cause, mental andphysical generals. There were no characteristics particulars. Opium a deep acting remedy was prescribed
in single dose.
Based on child’s hypersensitive emotional reaction and fast pace with good characteristics, dominantmiasm was Psora in this case. There was complete improvement of symptoms and signs within 4 days.Follow-ups until till three months did not reveal any relapse.
Case 2
A17year old female came with complaints of gradual onset of edema, Oliguria, proteinuria, hypertension 150/80 and ascites since 15 days.Patient as a person is mild in nature, obeys everyone and does everything to help all those who ask for help. She had delayed menarche and physical generals of aversion to milk and thermally hot. She was shy during interview. Her mother commented that she was the most affectionate of all the siblings.
Totality:
- Mild
- Yielding
- Bashful
- Affectionate
- Hot
- Aversion milk
- Delayed menarche
Discussion:
In this case, the patient has been to another homoeopath and was treated for 1 week with Apis 200 based on her presenting complaints. The remedy helped her initially and later the response had stopped. She was referred because the response to Apis had stopped. A deep acting remedy had to be released, based on the form which had mental and physical generals but no characteristics in particular. The remedy was Pulsatilla 200 which matched her mind and physical symptoms. More so, Pulsatilla is also a complementary remedy to Apis.
Pulsatilla 200 single dose was given. There was improvement of symptoms within a week, follow-ups were maintained till one month to ensure no relapse of symptoms. In this case we see a simple strategy of using a complementary remedy that completes the action of first remedy after the first remedy has stopped acting favorably.
Case 3
A boy who is aged five years, presented with complaint of edema, hypertension 140/90 and Proteinuria4+. Complaints started gradually, with a progress of 10 days duration. Along with AGN child complained of cough in short and dry bouts with dyspnea <midnight and lying down. He is originally irritable by nature and cannot tolerate anyone scolding him, and rather dominates others. He is hot thermally and craves sweets. Totality of the case is:
- Irritable
- Egoistic
- Dislikes scolding
- Dominating
- Hot pt.
- Craving sweets
- Mucus membrane
- Kidneys
- Bronchus
Discussion:
The boy is suffering from acute respiratory complaints and acute glomerulonephritis condition at the same time. Susceptibility expressed through a form for respiratory characteristics, cough aggravated midnight after and lying. Since susceptibility had thrown a characteristic form it had to be addressed as presenting symptoms, hence Ars-iod was prescribed first. Once the cough settled with Ars Iod in 2 days the deep acting remedy Lycopodium was prescribed which took care of the AGN.
It was important to note that AGN presentation had no characteristic form,hence adeep acting remedy based on mental and physical generals had to be prescribed in spite of acute presentation of the disease. Here the susceptibility and sensitivity reactions were good as characteristics symptoms were present in the case. A single dose of Lycopodium was prescribed. The miasmatic understanding is Sycotic, based on the slow onset and progress over ten days with no complications. There was improvement of symptoms in the patient within 4 days; follow-ups were maintained until three months and there was no relapse of symptoms.
Case 4
A 17 year old male came with complaints of gradual edema all over the body, blood pressure of 150/90mm Hg, proteinuria3+, haematuria2+, dyspnea and split s2. Duration of illness was 10 days. There were no other characteristics at kidney level.
In premorbid state child had no desire for mental or physical work, obstinate by nature, felt bad if he was scolded in front of others, has no courage to speak in front of others. He had fear of ghosts and dreams of ghosts. He had craving for sweets and pica. Chilly thermally.
Totality:
- Slow lazy
- Dislike for mental labor
- Sensitive to reprimands
- Lack of courage
- Obstinate
- Fear of ghosts
- Dreams of ghosts
- Craving sweets, pica
- Water logging.
Discussion:
In this case too, there were no characteristics symptoms of renal disease thus, no characteristics particulars as in previous case. So, based on the totality, the deep acting remedy –Calcarea Carb 200 was prescribed. Single dose was given, but there was no change in symptoms. Re-assessment of Miasm helped solved the issue of no registration of single dose of Calc Carb.
If we try to understand the case with ten days of duration sustained blood pressure, dyspnea and split s2, but no complications of LVF and ARF, it demonstrates a slow, sluggish yet unrelenting system. The case demonstrates low sensitivity with slow pace of evolution. There was slowness of the entire system during premorbid and morbid state. Slowness and obstinacy indicated a lurking Sycotic Miasm. There was need to push this sluggish system further as, registration was expected to be slow due to the very nature of Miasm. Three doses of Calc Carb 200 were given which did the trick. There was gradual improvement of symptoms in 9-10 days, follow-ups were maintained till two months and there was no relapse. This case demonstrates a typical SycoticMiasm activity slow to evolve, slow to react to homeopathic drugs and slow to resolve.
Case 5
An11 year old boy presented with complaints of edema grade 3, hypertension 170/90mm of Hg and proteinuria3+, which are of fluctuating nature. The duration of illness was 7 days but the complaints had developed rapidly in first 48 hours. As, there were no characteristics, once again we relied on premorbid attributes of the child.
The boy looked very hard and rough, and had no manners while talking to elders, very naughty, never bothered about others, will not allow others to touch his things. He was thermally hot and had cravings for meat /pungent.
Totality:
- Hard, rough look
- Insensitive to others
- Morals low
- Fear dark/alone
- Anxiety of losing his possessions
- Carving meat/pungent
Discussion:
The case expressed through inconstancy, there was blood pressure reaching up to 170/90 mm Hg and yet fluctuating. Pace of the disease was rapid with complications just setting in. All this was pointing towards a Tubercular Miasm in back drop.
Initially the deep acting remedy Calc Flour 200 was released, but it did not give any relief, hence, the remedy Tuberculinum as anti-miasmatic was released followed by the deep acting remedy Calc Flour 200 the next day.
Sensitivity of the child was suboptimal as suggested by his behavior patterns;the child was rough and unpolished. There were no characteristic particulars, indicating low sensitivity in morbid state. No characteristic particular at all, coupled with progressive disease, indicated a low responsive susceptibility.
In this case there weree two issues which had to be addressed, one being the Miasm, the other being the low susceptibility. Timely and aggressive intervention was required to prevent the case slipping off. Hence, as soon as the indicated deep acting failed to register an intercurrent remedy was released. This was followed by reintroducing the deep acting remedy in multiple doses to addresses sub optimal sensitivity & low susceptibility. The regime of anti-miasmatic followed by a constitutional helped in an acute disease presenting with low susceptibility in Tubercular Miasm.
The improvement was gradual in 9-11days. Once the patient showed sustained improvement over 4 days, a constitutional remedy was weaned off and patient was put on placebo for rest of observation period. Follow ups were maintained until three months. There was no relapse of the symptoms.
Case 6
A 5 year old female child presented with the complaints of edema grade 2, proteinuria4+, hematuria & hypertension 130/80.Associated with AGN was dry cough in short spells. She also had associated complaints of CSOM, Pyoderma, discharges were yellow in color. All the complaints started within 6 days. She as a person had multiple fears, of being alone and of darkness. Wants to be appreciated for her work, otherwise laments, irritable by nature and jealous. Thermally hot.
Totality :
- Fearful
- Fear of dark/alone.
- Jealous
- Lamenting when not appreciated.
- Irritable
- Hot pt
- Skin pyoderma
- Ear suppuration
- Yellow discharges
Discussion:
This child came with multiple issues all acute; cough, AGN, pyoderma and CSOM all starting a week ago. Respiratory complaint was most distressing. Based on the characteristic presentation of dry cough in short spells Alumina was prescribed.
AGN presented with proteinuria, hematuria and edema, and associated complaints of CSOM and pyoderma, indicate multiple pathologies with very few characteristics. Multiple inflammatory and suppurative pathologies (SKIN& CSOM) with moderate pace and no characteristic indicated a tubercular Miasm with moderate to low susceptibility.
Hence, after Alumina ameliorated distressing cough, Tuberculinum 1M single dose was prescribed as an anti-miasmatic treatment. Tuberculinum was not expected to cure the case, but it was supposed to facilitate the action of Calc Sulph which was child’s indicated constitutional remedy. Tuberculinum was followed by Calc Sulph 200 as deep acting remedy in infrequent doses. There was improvement in the case in 9 days. Follow up was taken till one month, and there was no relapse of symptoms.
Thus, in this case, we see a low to moderate susceptibility with tubercular miasmatic activity handled by sequence of prescription. Alumina(Acute) followed by Tuberculinum (Anti Miasmatic ) followed by Calc Sulph 200 (constitutional) all in single to infrequent doses to clear multiple sets of pathologies existing at the same time in the child.
Case 10
A 10year oldmale child who came with complaints of edema grade 3, proteinuria 3+, hematuria, hypertension 130/80 and ascites. The duration of the presenting complaints was since 2 days.
As a person child was irritable by nature, and cannot bear others dominating or shouting at him; he looked as if he was confident but is not so. He cries aloud and had craving for pungent things, cold drinks and he was hot thermally.
Totality:
- Egoistic
- Irritable
- Confident front and coward within
- Loud weeping
- Hot patient
- Craving pungent and cold drinks.
Discussion:
Once again in this case we see a similar pattern; ascites has set in but there are no characteristics at the level of particulars. Rapid pace, and progressive disease without individual characteristics indicated low susceptibility with tubercular miasmatic activity.
Based on premorbid symptoms, Lycopodium 200 was prescribed as the deep acting remedy. The response with Lycopodium was short amelioration with fluctuations in BP and other signs. Considering low susceptibility a trial was given to frequent repetition of Lycopodium doses.In spite of frequent repetition there was fluctuating response.
Based on the susceptibility which is in the low to moderate zone, coupled with tubercular Miasman anti-miasmatic remedy Tuberculinum 1M was prescribed in single dose. This was followed by the deep acting remedy Lycopodium 200 in multiple doses to bulldoze the case before it slipped out due to its inherent tubercular nature.
After a single dose of Tuberculinum the response pattern stabilized the fluctuation and response settled.There was improvement of symptoms with steadiness within 8 days. Follow-ups were maintained till two months, and there was no relapse. Lycopodium was weaned off after 4 days once the response pattern was established.
In this case we see repeated short ameliorations in a child with low susceptibility pattern in the tubercular Miasm. Though deep acting medicine produced ameliorations they would not last long. The disease would march forward after each short amelioration. The challenge was to balance the risk of marching disease and at the same time avoiding over stimulation with deep acting constitutional medicine. The risk was further amplified due to presence of tubercular Miasm which is known to be erratic and unpredictable in its activity. Hence, when susceptibility offered a small window period where response pattern was stabilized, the case was bulldozed before it could revert.
Case 7
A 11 old girl presented with complaints since 7 days of edema grade 2, proteinuria3+, hypertension 170/120 and occipital headache. She also had associated complaints are abdominal colic, loose stools, and tenesmus. Patient as a person cannot bear to be scolded, had fear of being alone and dark. Very affectionate to others, thermally chilly, craves meat and sweets.
Totality:
- Sensitive to reprimands
- Fear of dark
- Fear of being alone
- Affectionate
- Chilly
- Craving meat, sweet
Discussion:
In this case, we did an error by ignoring the characteristic form of colic, loose stool and tenesmus present as concomitant to AGN. Until now with the form with proteinuria, edema and hypertension, the prescribing pattern was deep acting remedy, so we prescribed the remedy as Calc phos. But, the remedy did not register. We soon realized we missed the bus. In all other cases we had observed that there is no renal system characteristic form, but to our surprise, in this case there was one. During case review we observed that we neglected a well-developed form of concomitants. It was a bad miss.
There was presenting complaints with characteristic particulars and concomitance and association, which include the sphere of action on GIT, Kidney and Congestion of circulatory system. Based on the association of symptoms of GIT colic with mucus and tenesmus associated with high blood pressure, congestive headache, in kidney affection Terebinth 200 was selected.
Terebinth, as acute remedy, in single dose was prescribed whic, brought prompt relief. It was followed by constitutional remedy Calc Phos to complete the cure. There was improvement of symptoms within 6 days.Follow-ups were maintained till four months without a relapse.
Nature has a surprise up its sleeves for everyone. Just when you feel you have understood the prescribing pattern based on assessment of susceptibility and Miasm in homeopathy, a surprise awaits us in the form of an exception. With humility andgrace we embraced it.
Case 8
8 year old female presented with signs and symptoms of edema grade 1, proteinuria+, hematuria+, and hypertension 160/100, loud S3 Audible with coarse crepitation in chest. All the complaints progressed within 2 days duration. The associated complaints were dry cough in short bouts, which is increasing during midnight.
She as a person had fear of darkness, animals and being alone. She felt jealous of others, cannot tolerate others if they won’t listen to her and try to dominate her. She is very irritable with violent shades of anger. She gets dreams of funeral, thermally hot and has craving for sweets.
Totality:
- Fear dark
- Fear of being alone
- Fear of animals
- Irritable from contradiction
- Violent anger
- Jealous
- Dominating
- Egoistic
- Dreams of funeral
- Hot
- Craving sweets.
Discussion:
In this case the pace of the disease is too fast, with complications setting in early, patient with S3 audible and high BP is on the verge of going into left ventricular failure. Along, with that the patient has acute dry cough with short bouts <midnight with RS examination findings revealed coarse crepitation. On close observation one notes that edema is Gr I, proteinuria is Gr I and so is hematuria yet, the cardiovascular system is in overdrive.
From Miasmatic angle this case is lurking in transition between tubercular and syphilitic zone. There is risk due to cardiovascular overdrive and lurking tubercular-syphilitic miasmatic zone; the case might easily slip into complications like encephalopathy or LVF. Nevertheless, the good thing is there are a good number of characteristics at the mental, physical general and particular level.
In view of early of cardiorespiratory involvement, Syphilitic Miasm and midnight aggravation,Ars.iod 200 was given as the choice of the remedy in this condition. After the acute condition settled and cardiac overdrive calmed down, Lachesis 200, constitutional remedy was prescribed to complete the cure. Lachesis is an anti- syphilitic remedy which covered the mental symptoms and physical generals of the case; incidentally it is also complementary to Arsenic. Due to presence of a good number of characteristics, the 200 potency in single dose was prescribed. There was recovery of signsand symptoms in 6 days. There was follow up for 2 months. No relapse of symptoms.
| Homoeopathic Therapeutic Strategy Table | |||||||||||||||
| Case # | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |||||
| Acute Remedy | Ars | Alumi | Terebi | Ars | |||||||||||
| Iod | na | nth | Iod | ||||||||||||
| Chronic Remedy | Opi | Puls | Lyco | Calc | Calc Fl | Calc S | Calc P | Lach | Nat | Lyco | |||||
| um | C | M | |||||||||||||
| Ant miasmatic Remedy | TUB | TUB | TUB | ||||||||||||
| Potency Acute Remedy | 200 | 200C | 200C | 200C | |||||||||||
| C | |||||||||||||||
| Potency Chronic | 200 | 200 | 200 | 200 | 200C | 200C | 200C | 200C | 200 | 200C | |||||
| Remedy | C | C | C | C | |||||||||||
| Potency Anti- Miasmatic | 1000C | 1000C | 1000C | ||||||||||||
| Remedy | |||||||||||||||
| Repetition Acute | 3 | 3 | 1 Dose | Multip | |||||||||||
| Remedy | dose | Doses | le | ||||||||||||
| s | |||||||||||||||
| Repetition Chronic | Sing | Sing | Singl | 3 | Frequ | Infreq | Single | Single | 3 | Frequ | |||||
| Remedy | le | le | e | dose | ent | uent | Dos | ent | |||||||
| s | es | ||||||||||||||
| Repetition Anti- | Single | Single | Single | ||||||||||||
| miasmatic Remedy | |||||||||||||||
| Dominant Miasm | Pso | Syc | Syco | Syco | Tuberc | Tuberc | Tuberc | Tuberc | Syco | Tuberc | |||||
| ra | osis | sis | sis | ular | ular | ular | ular to | sis | ular | ||||||
| Syphili | |||||||||||||||
| tic | |||||||||||||||
| Strategy | CH | AC – | AC – | CH | CH -> | AC- > | AC -> | AC -> | CH | CH -> | |||||
| Acute(AC)/Chronic(CH)C | > | > CH | IC | IC-> | CH | CH | IC -> | ||||||||
| omplimentary (CO) Anti- | CO | CH | CH | ||||||||||||
| Miasmatic (IC) | |||||||||||||||
| Recovery | |||||||||||||||
| 0-4 Days | 4 | 4 | |||||||||||||
| 4-8 Days | 6 | 6 | 6 | ||||||||||||
| 8-12 Days | 10 | 11 | 9 | 8 | |||||||||||
| 12-18 Days | 15 | ||||||||||||||
| Follow Up Duration in | 3 | 1 | 3 | 2 | 1 | 1 | 4 | 2 | 1 | 2 | |||||
| Months | |||||||||||||||
| Relapse | NIL | NIL | NIL | NIL | NIL | NIL | NIL | NIL | NIL | NIL | |||||
Versatility is the key to managing the complexity of homoeopathic treatment in Acute Illnesses such as AGN. Thorough grounding in fundamental subjects of medicine, pathology, Organon of medicine and Materia Medica provide the launching pad for a homoeopathic physician to be versatile in practice.
CONCLUSION:
- Homoeopathy offers an effective and uncomplicated solution to the problem of Acute Glomerulo Nephritis with comparable or better outcomes as compared to conventional therapy.
- The principle of individualization remains the central theme for management of AGN in pediatrics. Scope of individualization has to expand to include not just the symptoms of patients but also the pace and stage of disease, clinic- pathological correlation, and quantitative assessment of susceptibility and qualitative judgement ofMiasm.
- Clinical observation of this study suggests that barring less than 20 % cases, almost all susceptibilities (individuals) did not throw characteristic particular symptoms (characteristic urinary tract symptoms) in the entire evolution of the disease.
- Most casespresented with common diagnostic symptoms of odema, proteinuria, hematuria and hypertension. Due to this peculiar trend of symptomology, individualization had to be based on per morbid constitutional attributes of the children.
- Remedy Selection in all the cases were based on understanding of symptomatology e.g. presenting symptoms, association of symptoms, pre- morbid attributes of patients etc. In short,the combination of symptoms presented by patient decided the individualistic homoeopathic approach.
- Going by the principle of individualization and respecting symptomatology patterns; Apis, Acetic acid, Apocynum, Natrum Mur, Cantharis etc. got vetoed out which are used more commonly as remedies in kidney disorders.
- As in this study, most cases, lacked florid characteristic symptoms of renal origin, hence understanding of pace of disease, stage of pathology and assessing evolution pattern of symptoms formed a vital trio to access dominant Miasm.
- This study revealed cases exhibiting all four Psora, Sycosis, Tubercular and Syphilitic Miasmas. Tubercular Miasm was most frequently encountered followed by Sycosis, Psora and Syhilitic Miasm as dominant in expression.
- Countering the Tubercular Miasm menace was an important strategy in resistant cases or those on the verge of life-threatening complications. The anti-miasmatic remedy Tuberculinum played a decisive role in facilitating cases which experienced miasmatic block, indicated by repeated short ameliorations or slow or non-registration of indicated homeopathic constitutional remedy.
- Management Strategy includes selection of first prescription, second prescription, potency and repetition. In most cases, constitutional drug was prescribed even though AGN is acute in nature. This had to be done because of the depth of pathology and multisystem involvement in a miasmatic illness. In addition, cases did not present with characteristic particular symptoms of kidney for acute remedies to get indicated.
- Cases which presented with characteristic particulars and concomitants were respected as in cases where Alumina, Ars.Iod and Terebinth were used as first and second prescriptions based on presenting acute totality.
- Posology and second prescription decisions such as selection of potency and repetition, introduction of anti-miasmatic remedy were based on assessment of Susceptibility, 2.Dominant Miasm3.Remedy Reaction .
- Most cases responded to single doses in moderate potency because pre- morbid characteristic symptoms were available to build constitutional totality. A small group of cases required repetition of doses mainly to counter the low responsiveness of susceptibility to homeopathic stimuli.
- SinceAGN is a rapidly progressive disease with life threatening complications like Encephalopathy, LVF and ARF, observation periods on placebo were relatively short especially in cases with dominant Tubercular and Syphilitic Miasms.
- For studies of diseases which are acute in nature with life threatening complications a cross-functional team of doctors is essential.
- Standardized recording system is absolutely essential for primary recording of case data. Homoeopathic Software “Organon 96” was used for systematic documentation and comprehensive analysis.
References
- (n.d.). In TEXT BOOK OF MEDICINE 6TH EDITION.
- Boericke, W. (n.d.). In A handbook of Homoeopathic Materia Medica.
- Boger, C. M. (n.d.). In A Synoptic Key to Materia Medica.
- Burt, W. H. (n.d.). In Physiological Materia Medica.
- Clarke, J. H. (n.d.). In A dictionary of Homoeopathic materia Medica.
- Cotran, R. (n.d.). In Pathologic Basis Of Disease 9th Edition .
- (N.D.). In Principles And Practice Of Medicine- 20th Edition.
- Dhawale M.L. (n.d.). PsoraSyphilis: miasmatic interpretation and clinic-pathological correlations with
comparisons. In C 5,Area C: Perceiving miasmatic evolution, ICR Symposium volume on Hahnemanniantotality, Part I, 3rd edition.
- Kasad K.N. (n.d.). Disease (Natural and drug):A phenomological approach, C1. In Area C: Perceivingmiasmatic evolution, ICR Symposium volume on Hahnemannian totality, Part I, 3rd edition.
- Kliegman, K. (N.D.). In Nelson Textbook Of Paediatrics 18th Edition.
- (n.d.). In S R. Materia Medica of Homoeopathic medicines.
- Samuel Hahnemann. (n.d.). In Organon Of Medicine, 6th Edition, Reprint Edition 2003. Ibpp Publishers.
Dr Kalyani Koya
M.D(Hom)
Assist Professor
Department of Community Medicine
JIMS Homoeopathic Medical College & Hospital
Navin Pawaskar
M.D (HOM), MICR (BOM), MHA(USA), CPDM(USA)
Healthcare Consultant
JIMS Healthcare



I found this an extremely valuable article. Drs. Navin Pawaskar and Kalyani Koya provide a an excellent model of how to proceed is such cases.