

The aim of this review has been realised, in that, by utilising homeopathic methodology, the genus epidemicus has been identified and subsequently six main remedies considered as being appropriate for treatment of the documented stages of the disease process from inflammation through to necrosis in susceptible individuals. The information reviewed concerns both the accepted theory and practice of treatment of the disease process in N.F. which can result in states of inflammation, suppuration, gangrene or finally necrosis as a consequence of puncture wounds (caused by drug injection), repeated over time or infected by an exogenous pathogen in those with a compromised immune system (C.I.S.), and the theory and practice in homoeopathy for treatment of similar states, with similar causes. This paper supports the assertion that homoeopathic treatment is a viable alternative when antibiotics are proving ineffective.
AIM
To identify a group of appropriate homoeopathic medicines, which can potentially be used in threatening or actual suppuration in abscesses and necrosis of same or other local sites, in susceptible individuals. In this review I consider particularly those of homeless status who are also intravenous drug users (especially of heroin).
OBJECTIVES
- To discuss risk factors which predispose some individuals to a lowered immune system who are therefore more susceptible to developing or contracting Necrotising Fasciitis (N.F.)
- To examine details of documented and possible bacteria involved in the process of suppuration leading to necrosis.
- To consider relevant homoeopathic philosophy in relation to susceptibility, maintaining causes, and predisposition.
- To outline the disease process involved which may lead in some individuals, to developing N.F.
- To present a resume of individualised homoeopathic remedies potentially suitable for use in all stages of the disease process outlined in Objective Four.
BACKGROUND
In June 2000, 22 drug users in Scotland and 21 between Dublin and Manchester (1), died after contracting (or developing) Necrotising Fasciitis, and again in July 2001 eight individuals were affected, either fatally or requiring surgical debridement and/or partial amputation. These cases were thought to be the result of using contaminated heroin for injecting in cases of drug addiction. (2) The condition itself is described as “… a rapidly progressive soft-tissue infection that involves superficial and deep fascia leading to thrombosis of cutaneous vessels and gangrene of underlying tissues.” (3) It was first documented by Fournier in 1883 (4), and Meleney isolated a particular bacteria as a causative factor in 1924. (5) The term ‘necrotising fasciitis’ was ascribed to Wilson, who, in 1952, noted that an “essential component” of gangrene with a specific bacteria, involved the deep fascia. (6) The condition can occur in any anatomical location, usually at a distance from any trauma but also at affected sites. Other names that it is known by e.g. Fournier’s Gangrene (genital), Meleney’s Ulcer or Hospital Gangrene etc., often indicate either anatomical sites or places where infection was contracted or developed. (7) Conventional therapy involves antimicrobial treatment with e.g. Penicillin, aminoglycoside, metronidazole etc. and Hyperbaric Oxygen Therapy (HBO) and surgical excision, including debridement and amputation when considered necessary. (8)

RISK FACTORS
There are several factors, which are conventionally regarded as leading to possible susceptibility in contracting or developing N.F. The greatest of these is that of having a ‘compromised’ immune system, which is noted in conditions such as; Diabetes Mellitus, malignancy, renal impairment and trauma. (9) In this discussion, which is intent on reviewing the specific factors in relation to the circumstances of intravenous drug users who may be homeless, two of the above noted conditions are worthy of further exploration. In the first instance, similar to Diabetes Mellitus II, where a state of ketosis may develop due to the inability of the body to utilise carbohydrates and glucose, it is worth pointing out that it is also possible for ketosis to develop in states of starvation or eating disorders. The result being, that fats and proteins become the primary energy sources, which may produce ketones in the blood, and thereby lead to ketoacidosis (10). In the report of a survey carried out in 1999 by the Office of National Statistics titled, ‘Health and Well Being of Homeless People in Glasgow’ published in June 2000,
“19% of respondents had eaten only once in the day prior to interview and 5% had not consumed any food at all. Fifteen per cent of respondents did not consume any hot food (excluding drinks) in the day prior to interview.”
It would seem probable that in such circumstances, it would be possible for heroin addicts who are also of homeless status to be at similar risk to developing a condition akin to ketoacidosis, which may also result in renal damage. In addition, it is well known that nutritional deficiencies play a decisive role in the prevalence and severity of microbial diseases in under privileged people. The rate of wound healing is also markedly influenced by dietary factors especially in deficiencies of some vitamins including Vitamins C, E, K, B6 and Minerals such as Calcium and Iron. (11)
The citing of ‘trauma’, as a further risk factor is particularly apt in the present examination of the incidence of N.F. in intravenous drug users. ‘Trauma’, here being defined as: “…any injury caused by a mechanical or physical agent.”(12)
Heroin addiction most often requires the use of intravenous means whereby the subjects repeatedly inject the drug, causing puncture wounds, often several times daily for, perhaps, a duration of some years, with little or any use of disinfecting measures. Thus creating a higher than usual risk of infection at multiple sites, most often on arms and legs but the groin area is also used amongst others, as more accessible veins become unusable.
START HERE
In the outbreaks of N.F. documented here, this is all the more relevant, for it has been discovered that all the cases had a significant factor, i.e. the injection has been made directly into muscle tissue or accidentally into other tissues when a vein has been missed. (13) . This assertion also brings to bear the immune inhibiting effects of drugs themselves as a risk factor to infection which include non-steroidal inflammatory preparations such as aspirin, ibuprofen, naproxen etc. that inhibit the inflammatory mechanism that makes tissue repair possible. Steroid use is particularly implicated, possibly due to the fact that cortisone interferes with the production of antibodies under certain conditions. This immunologic inhibition cannot account entirely for the infection enhancing effect. In addition to interfering with antibody production, cortisone influences many other physiologic processes, some of which may affect directly or indirectly the response of the body to infection. Interference with the inflammatory response and with the activity of the reticulo-endothelial system, disturbance of the intermediary metabolism, and activation of proteo-lyctic enzymes (14) are but a few of the effects of cortisone that might be important in this regard.
The habitual use of heroin, (the popular name of diacetyl-morphine, a semi- synthetic compound derived from morphine and stronger than the natural drug), which has its effects principally on the Central Nervous System (CNS) and also affects some peripheral organs such as the alimentary tract and the respiratory system, is a definite factor in compromising the immune system. Morphine usually neither eliminates the psychological perception of pain nor blocks the sensation. Although there are exceptions, the person knows that pain continues, but he or she is not disturbed by it. The associated fear and tension subside so that the pain becomes bearable. These reactions signify the effects on the CNS but the opiates may also change the activity of peripheral nerves that conduct messages to and from the brain. The enkephalins involved are found in neurons in the spinal cord and portions of the hind and mid-brain which transmit pain and related sensory signals (for example, heat and cold), and in parts of the mid-brain associated with movement, mood and behaviour. The enkephalins are also found outside the central nervous system in the neurons of the periphery and the gut. (15) These effects have relevance in two areas in connection with this investigation: the fact that the addict despite feeling hunger is able to ignore these feelings. This can result in the production of acids in the gut which having no food to breakdown will tend to become destructive to the alimentary tract itself. The other danger is that by being able to ignore sensations of heat, pain and even fear for health, any inflammation, abscess formation or numbness can continue unabated.
BACTERIOLOGICAL FACTORS
In the past, several types of bacteria have been identified as being involved in the presentation of N.F. On this basis, two types of N.F. had been labelled, i.e. i) Polymicrobial, involving a number of organisms in various combinations and ii) Pure group A Streptococcal, which is said to be haemolytic, (rupture of RBC membrane). (16) In direct relation to the cited outbreaks, Clostridiun Novyi Type A among others, was isolated from eighteen of the people who developed N.F. in June 2000. (17) Some of these bacteria are known as being indigenous (ie. present in a healthy state) to the human body, e.g. Bacteroides, Staphylocci, Streptococci, Pseudomonas aeruginosa, Clostridium etc.
Two aspects are known to be observable concerning these micro-biota:
- That most micro-organisms commonly harboured by the body in a state of health are capable of exerting a wide range of pathological effects under special conditions and,
- Many of the micro-organisms classified as pathogens, indeed probably all of them, often persist in vivo without causing overt disease. (18)
As has been previously noted, nutritional deficiencies, exposure to toxic agents, and certain kinds of physiological stress are among the many causes of disturbances associated with disease processes caused by indigenous microbiota. In other words, some form of pathological or at least abnormal state must exist before indigenous bacteria can multiply to such an extent that it causes deleterious effects. George Bernard Shaw echoed Pasteur who suggested that a physiological disturbance might in certain cases be the primary cause of the infectious process rather than its consequence, when he said: “The characteristic microbe of a disease might be a symptom instead of a cause.” (19) Early in the investigations of 2000, Dr Laurence Gruer, Consultant to the Greater Glasgow Health Board commented that:
“It is quite possible that no single cause for the illnesses will be identified. Many injectors in the affected areas of Glasgow have said that their recent supply of heroin has required unusually large amounts of citric acid to be added before it can be dissolved for injecting. A variety of different bacteria normally found on the skin have been isolated from tissue or blood from several patients. It is likely that injection of the unusually strong heroin and acid mixture can cause severe damage to muscle and other tissue. This may then create the conditions for harmless bacteria present in heroin or carried on the needle from the skin to cause serious infection.” (20)
Clostridium Novyi, Type A, was isolated in some, though not all, recent or current cases of N.F. at the time and described as an “…’anaerobic’ bacteria-that is, they only grow in the absence of oxygen (dead tissue). Some Clostridium can not only cause severe infection in damaged tissue but can also produce very powerful toxins. They can also exist in for years in dust or soil as dormant spores, only becoming activated when the conditions are right.” (21) But it was only previously been known to cause serious infection in domestic animals; very rarely in humans and is commonly found in soil and animal faeces. Other types of Clostridium have been located in intestinal flora of the human where it is non-spore forming.(22)
It is therefore a matter of postulating whether the Clostridium isolated in the cases cited, is the actual cause originating in contaminated heroin supplies and therefore exogenous. In classical infections of exogenous origin, the determining etiological event of the disease is said to be exposure to the infective micro-organism. This was yet to be made clear in the present situation. The author has been unable to locate documentation on this particular strain of Clostridium (ie. Novyi) in standard textbooks on microbiology and this raises two questions:
- In which conditions, if any, has it been previously been isolated?
- Or, is it a possible new mutation arising from this particular combination of factors met in this incidence of drug injectors?
In indigenous microbial disease, the immediate cause is the environmental factors that upset the biological equilibrium normally existing between the host and the microbial agents.The documented factors common to many (but not all) of the affected were:
- They are all Heroin Injectors, whose supply source may or may not have been the same.
- Many, if not all, used more Citric Acid than usual to dissolve the drug for injection.
- The subjects all injected into muscle or tissue other than a vein.
If the source of supplied heroin was the same and all users of this supply increased the quantity of Citric Acid – plus the involvement of the injection into muscle and other connective tissue, (which is not particularly uncommon in heroin addicts), not all heroin injectors likely to have used this batch of the drug under these circumstances, have succumbed to either infection or development of N.F. It would have to be considered somewhat as a result of this combination of factors or it would suggest another unidentified predisposing factor. Dr. Jai Lingappa, Epidemic Investigation Officer at the Centers for Disease Control in Atlanta, commented that:
“A lot more work still needs to be done to clarify how exactly the Clostridium Novyi is contributing to the illness……..We also want to learn more about why these people became sick and others didn’t.”(23)
The purpose of reviewing this serious condition, (N.F), with the prospective use of Homoeopathic medicines for treatment in mind, is to put forward an approach that will to a degree bring into congruence the determinants of infection and the determinants of disease and present a means of treating the pathological processes which can ensue from both exogenous and indigenous causes, and to understand and control the processes responsible for converting so-called infection into overt disease. This approach is found in Homoeopathic philosophy and practiced in the homoeopathic treatment of both individuals and genus epidemicus. Relevant theory is summarised in the next section.
MIASMATIC FACTORS
Even from the viewpoint of conventional medicine, a person in robust health may easily resist exposure to even the most virulent microorganisms. The degree of resistance can change from hour to hour and day to day depending upon exhaustion, starvation, cold, overwork, emotional stress, etc. It has been stated clearly in a standard textbook on microbiology used in all universities and medical schools in the U.S., that the susceptibility factor is so significant that it is virtually impossible to decide the infective dose of a specific microorganism. (24) In the cited cases of those developing N.F., this study has identified at least some of the major factors related to increased susceptibility to developing a seriously life threatening infectious disease and this is further explained in Homoeopathic philosophy by considering not just the ‘compromised’ immune system but by also considering the effects on the Defence Mechanism of the human organism. This defence mechanism is known in homeopathy as the Vital Force and is considered in terms of electro-dynamic vibrations, which involves a great degree of complexity.
“The vital force level of the human organism is considered the dynamic plane, affecting all levels of the being at once with varying degrees of harmony and strength. It is a highly complex, fluid, flexible, and energetic process, simultaneously responding to and affecting the surrounding environment……The whole organism, and any component of it, can be strengthened or weakened depending upon the degree of harmony, resonance, and force of the morbific or therapeutic influence applied to it.”(25)
When the strength of a noxious trigger is stronger than the strength of the vital force, the defence mechanism is called into play to counteract the stimulus. If the vital force is so weakened by exciting and maintaining causes, any powerful noxious trigger would alter the state of the entire organism without adequate defence, and death would rapidly ensue. There is a latent period before actual symptoms develop, during which the defence mechanism begins to adjust to the effect of the stimulus. In bacterial infections this ranges from hours to days.
From this premise it should be clear that disease is a result of a morbific stimulus which resonates with the particular susceptibility of the organism. This stimulus is known as the exciting cause and may be a microorganism, a foreign chemical, an emotional shock, a vaccination, etc.
Maintaining causes are those factors external to the organism which, because they continue to affect the individual over a period of time, maintain the individual in a weakened state eg. Lack of nutrition, unsanitary or damp living conditions, drug addiction; conventional drugs prescribed for long periods or repeated often in short periods of time (also regarded as Iatrogenic miasms), repeated emotional trauma, in short, many of the factors previously mentioned. But yet, the predisposition underlying much of these areas of susceptibility is the Fundamental Cause.
“Useful to the physician in assisting him to cure, are the particulars of the most probable exciting cause of the acute disease, as also (are) the most significant points in the whole history of the chronic disease to enable him to discover its fundamental cause, which is generally due to a chronic miasm. In these investigations, the ascertainable physical constitution of the patient, his moral and intellectual character, his occupation, mode of living and habits, his social and domestic relations, his age,… etc., are to be taken into consideration.” (Para. 5, The Organon of Medicine, Samuel Hahnemann, 5th & 6th Edition, B.Jain Pub. Reprint 1992)
The theory of Chronic Miasms is complex and involved and it is not within the scope of this review to give a full explanation of such. (Please see Bibliography section for further study). In summary, it is sufficient to say that a miasm is a resulting stereotypical disease condition, sometimes heredotransmissable, which can be latent or active, acute or chronic. Nevertheless, it is always the result of both a maintaining cause (hence the lingering disposition) and an exopathic exciting cause (the noxious trigger).
There is one miasmatic pattern, relevant to this review that has been recognised for most of Homoeopathy’s history ie., the Luetic Miasm. This particular pattern is in essence one of destruction and disintegration. There will often be a predilection in the family history to similar patterns of destructive illnesses, eg. Syphilis, alcoholism, conditions where ulceration has taken place or a tendency to necrosis, etc. When active and predominant in an individual, this pattern will taint and distort expression at all levels, mental, emotional and physical. In the individuals involved in the outbreaks of N.F. cited , the destructive pattern is essentially seen in addictive habits concerning the use of heroin and often several other substances. There exists a craving for acidic or spicy foods in general, there is a metabolic tendency to acidity and they are often of a temperament conducive to states of rage; that is when not suppressed by drugs. The effects of this pattern whereby heroin addiction is a symptom result in destruction not only of the immune system and particular bodily organs and systems e.g. the heart and circulatory system, but as noted, affects the intellectual faculties, the emotional responses and subsequent behaviour destroys family and social contact.
With regard to the ‘contagious principle’, Hahnemann, (1755-1843, founder of Homoeopathy), though not having the benefit of a microscope, put forward an uncannily accurate explanation more than half a century ahead of Robert Koch and others. He suggested in 1832 (Lesser Writings, p.758) that cholera, for instance, was caused by “…an enormous …brood of excessively minute, living creatures.”
He also regarded each epidemic (acute miasm) as having features of its own (the genus epidemicus) And since it is always the product of a single cause it will, in all individual cases, be amenable to one and the same specific remedy, the epidemic’s simillimum. (26)
THE DISEASE PROCESS
In this section, the disease process taken into account is that which begins, for our purposes, from the available information on the circumstances and states of individuals who were involved in cited presentations of actual or threatening N.F.
They are individuals who are:
- Intravenous Drug users i.e., heroin injectors;
- Experience a chaotic lifestyle, which often includes bouts of homelessness.
- Deaths predominantly in females. (27)
In the first assertion, two factors are particularly important:
1a). Lowered Immune System due to chronic heroin use (poisoning);
1b). Bodily subjected to repeated trauma from puncture wounds.
In the second assertion, two factors are again considered of import:
2a). Immune system further compromised by chaotic lifestyle, especially during times of homelessness, resulting in:
- Reduced intake of adequate food and nutrition.
- Exposure to the elements.
2b). Less access to medical services when required, unless in an emergency.
This information provides some clues to the degree of susceptibility at the general level of health and the particular susceptibility at the physical sites by repeated trauma and risk of infection.
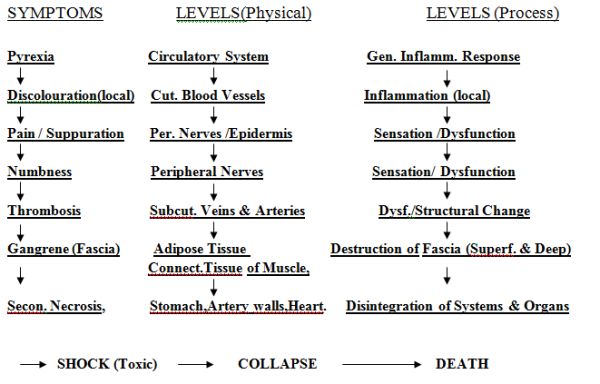
Schematic Evolution of Possible Disease Processes in General Terms
- Comp. I. S. –> Repeated Puncture Wounds –> Abscess Formation –> Necrosis of tissue at local sites with possibility of developing N.F.
- Comp. I.S. –> Vein injection infected by exogenous pathogen –> Septicaemia –> Possible development of N.F.
- Comp. I.S. –> Injection into Fascia, infected by exogenous pathogen and/or high levels of acid at site creating environment for mutation of indigenous bacteria. –> Rapid development of N.F.
Schematic Evolution of Disease Processes through Particular Levels and Systems
This section is based on available information from previous documentation and current GGHB Bulletins.
The following section is adapted from ‘Thorsons Encyclopaedic Dictionary of Homoeopathy’ by Harald Gaier. (Pgs. 130-132, Pub. Thorsons,1991) due to its admirable scientific clarity.
DISEASE and DRUG ACTION in HOMOEOPATHIC CONGRUITY
Applied therapeutic science requires a coincident parallelism between the symptom complexes of both the disease and the drug of choice on as many of the first seven under-mentioned points of comparison as possible. Obvious incongruity in any comparative aspect frequently amounts to symptom dissimilarity in the case, allowing for the elimination of many otherwise eligible remedies, facilitating the process of repertorisation.
- 1. Generic Similarity
Homoeopathicity of type of affliction; describes the identity in the class of affections induced by both the natural disease of the patient and the experimental disease of the drug to be used: eg. I) if the illness is febrile, the remedy must be pyro-genetic; ii) if the disease is an inflammation, the drug of choice will be an irritant, etc.
- Causal Similarity
Homoeopathicity of formative affectors; means that the antecedent concomitants present when the disease arises will substantially narrow the field of contenders among drugs to be used: eg. I) neuralgia induced by injury to a nerve is different from one brought on by shingles and that again is also distinct from one that comes on with gout.
- Parallels in Symptom Modalities
Homoeopathicity of modalities. Meteorological and thermal influences, cosmic rhythms, mental factors, physical conditions (including movements and rest), relation to food and drink, location, laterality and time are circumstances that can contribute to making symptoms I) better or ii) worse, iii) appear or iv) change.
- Symptom Character Resemblance
Homoeopathicity in the quality of abnormal sensations. All sensations have a distinct character: for instance, a gnawing pain, a burning pain, a tearing pain etc. are distinctly different from each other. The character of such sensations are to be alike in both the disease and the drug action.
- Constitutional Compatibility
This describes the aggregate of patients’ common features. It is used to identify patients according to their temperament, appearance, certain characteristics of behaviour and their variance from the normal, which should be compatible with the corresponding remedy.
- Synchronicity of Symptom Evolution
Homoeopathicity of pharmocodynamic devolution; meaning that various developmental aspects of the disease process of the patient must synchronise with the developmental pathogenicity inherent in the drug to be applied.
- Concordance of Emotional Symptoms
Homoeopathicity of disposition; matching emotional and/ or the intellectual symptoms. Since mental and emotional symptoms are in evidence well ahead of functional and morphological changes when disease develops, they frequently provide very early indications for homoeopathic treatment.
- Matching of Three or More Guiding Symptoms
Multiples of semiological homoeopathicity. Reliance on the coincidence of three, but preferably more, striking symptoms, evident in both the artificial illness of a drug as well as in the phenomena of a disease, rests on the mathematical law of permutations. If three distinctive symptoms of a case can be found to have been experimentally produced by a medicine, there is already considerable likelihood of its acting on the same parts and in the same manner.
- Ranking
Many homoeopaths are guided by Robert Gibson Miller, who in 1910 proposed ranking the above points of comparison in the following order of priority:
- matching mental & emotional symptoms;
- correspondence between modalities of time, season, motion, locality, sensation etc.
- similarity of pronounced cravings and aversions;
- menstrual, or hormone-related, changes in state in both the natural and the artificial diseases;
- resemblance between the particulars as well as the generals of both diseases, where only the peculiar, unexpected, striking or unaccountable symptoms are of significance;
- common symptoms, as featured in standard non-homoeopathic disease classifications.
The Simillimum is the medicine, which in its manifestations most clearly reflects the total symptom picture of the individual’s diseased state, which will certainly cure that patient, if the patient’s condition is within reversible limits. (28) In relation to the symptoms available from the documentation in the author’s possession, which have little or no individuality, it is less likely that the most accurate simillimum will be found. But as will be explained, it is not always the best remedy to prescribe even if it were possible (ie, by taking information from those who are displaying symptoms associated with the recent outbreak or who are thought to be at greatest risk.)
Contra-indication Against Administering Simillimum
In a patient, whose disease is terminal and which may be in its final stages, namely where the life force is hopelessly overwhelmed by the forces of disease, or in many emergencies, it is absolutely contra-indicated to prescribe the individual’s simillimum, which would, in these circumstances, only be able to produce an aggravation hastening death. In such an instance functiotropic, organotropic or pathotropic remedies ought to be the homoeopathic drugs of choice, with the intention of inducing a measure of improvement for the limited period remaining to the patient.(29 Therefore, the remedies identified by using predominantly common, general and particular symptoms which have no modalities, will be sufficient when given at the appropriate phase in the disease process and may reflect more the nature of the Genus Epidemicus rather than the simillimum of the individual patient.
FINDING THE GENUS EPIDEMICUS
Although, it is not as yet possible to find, or would in some cases be inappropriate to utilise the simillimum, many of the above mentioned principles will still be employed to find the remedy or remedies that come closest to the picture of the genus epidemicus. This means that, depending on at which stage of the disease process the remedy is administered, there is a possibility of preventing the development of N.F. or reducing the effects of infection before it reaches a life threatening degree.Symptoms will be taken from all general and particular disease processes outlined above:
Repertorisation using Synthesis (R.H.S.) Edition 5.2 Edit. Dr. Frederick Shroyens
GENERALS:
Wounds: 1.Penetrating (Punctured) +.Stab wounds, Synth.Pg.1720; APIS, Arn, Carb-v, Cic, Hep, HYPER, lach, LED, Nit-ac, sil, sulph.
2.Bluish + Black, Synth. Pg.1719; Apis, China, LACH.
3.Suppurating, Synth. Pg 1720; Arn, asaf, Bell, Calc, Calen, Cham,Chin, Hep Lach, Led, Merc, Sil, Sulph
4.Dissecting, Synth. Pg.1719; Anthraci, Apis, Ars, kreos, Lach, Led, Pyrog.
5.Gangrene of, Synth. Pg.1719; Anthraci, ARS, Bell, Calen, Carb-v, China, LACH, sil,vip.
Inflammation: 6.Wounds, Synth. Pg.1619; Arn, hyper, lach, led, sulph.
7.Gangrenous, Synth. Pg.1618; ARS, bapt, Carb-v, hep, Iod, kreos, LACH, merc, Phos ,SIL
Abscesses: 8.To abort, Synth.Pg.1547: Apis, arn, bell, bry, calc, calc-s, hep, merc.
9.Absorption of pus, Synth.Pg.1547; Iod; LACH; Phos; Silicea
10.Gangrenous; Ars; asaf; carb-v; chin; hep; kreos; LACH; merc; nit-ac; phos; sil.
FEVER
- Septic; Synth. Pg. 1487: ANTHRACI; Apis; ARN; ARS; BAPT; Bell; BRY; Carb-v; LACH; Merc; PHOS; PYROG; SULPH.
- Zymotic; Synth.Pg.1490: Anthraci; apis; ARN; ARS; BAPT; Bell; BRY; carb-v; hyos; ip; LACH; Merc; op; Phos; Puls; Pyrog; Sulph.
MIND
13. Morphinism: Synth. Pg.152; Ars, bell, calc; cham; hyos, ip, lach, merc, op; phos; puls.
Each remedy is rated by the number of rubrics in which it appears and by how prominent or characteristic it is in the remedy picture, ie. Those in CAPITALS, are given 3 points; Those in Italics, are given 2 points; and those in plain type are given 1 point.
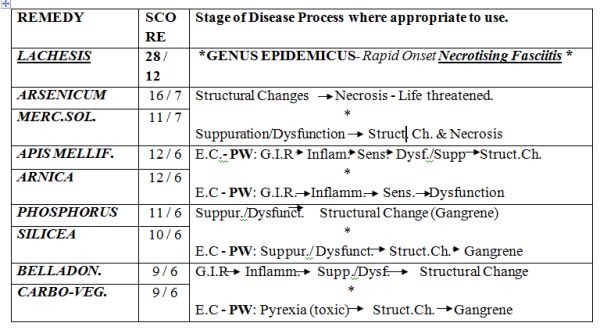
REMEDIES (present in SIX or more Rubrics) + Points Rating / No. of Rubrics
REMEDY |
SCORE |
Stage of Disease Process where appropriate to use. |
LACHESIS |
28 / 12 | *GENUS EPIDEMICUS- Rapid Onset Necrotising Fasciitis * |
ARSENICUM |
16 / 7 | Structural Changes Necrosis – Life threatened.*Suppuration/Dysfunction Struct. Ch. & Necrosis |
| MERC.SOL. | 11 / 7 | |
APIS MELLIF. |
12 / 6 | E.C.- PW: G.I.R Inflam. Sens. Dysf./Supp Struct.Ch.*E.C – PW: G.I.R. Inflamm. Sens. Dysfunction |
ARNICA |
12 / 6 | |
PHOSPHORUS |
11 / 6 | Suppur./Dysfunct. Structural Change (Gangrene)*E.C – PW: Suppur./ Dysfunct. Struct.Ch. Gangrene |
SILICEA |
10 / 6 | |
| BELLADON. | 9 / 6 | G.I.R Inflamm. Supp./Dysf. Structural Change*E.C – PW: Pyrexia (toxic) Struct.Ch. Gangrene |
| CARBO-VEG. | 9 / 6 | |
| KEY: E.C. = Exciting CausePW: = Puncture WoundsG.I.R. = General Inflammatory Response | ||
MATERIA MEDICA for GENUS EPIDEMICUS
LACHESIS
Source: This remedy is prepared from the venom of the viper, Lachesis trigonephalus, the Surucuccu or Bushmaster snake of South America. The venom is preserved dry or in glycerine.
Poisoning Symptoms: All the vipers are venomous; severe pain comes on at the site of a bite, bloody serous discharge and ecchymoses in the vicinity of the bite and thrombosis, followed, if not at once fatal, by local inflammation and sloughing, and even gangrene.
Swelling and black or purple discolouration of a limb may follow. Fever, with delerium and blood poisoning, sets in, followed by suppuration, haemorrhage or gangrene. Death may follow a bite from the following causes:
- If a vein has been pierced, quickly from thrombosis;
- after some hours from heart failure, through paralysis of the vasomotor centres;
- after a few days from secondary bleeding;
- later from septic infection of the necrotic area around the bite.(30)
Pharmacology: The venom of Lachesis contains a full range of potent enzymes, proteolytic, cytolytic, neurotoxic and coagulant. One or more of these effects may predominate. The blood is attacked primarily, while, the nervous system is at first aroused and excited. The main affinities therefore are with the blood, causing disintegration of red cells, lowered coagulability after initial tendency to thrombosis, and impaired resistance to infection with associated liability to gangrene and necrosis. Also the CNS, with ensuing delerium, coma and paralysis of vital centres. Also with the cardiovascular system as evidenced by hypotension, cold sweats and collapse. (31)
Therapeutics: The great blood-disintegrating (haemolytic) powers of Lachesis are utilized in a number of febrile, septic, toxic and typhus-like conditions, present in many named diseases, and in some forms called ‘malignant’ exanthems, where the body resistance has more or less completely broken down. When this point is attained the distinguishing or diagnostic features of the particular diseases have largely disappeared. As a Professor Teale, in a lecture before the British Homoeopathic Society, explained: “Widely different bacteria may produce very similar clinical features… when profound poisoning occurs, instead of the poisoning becoming more, it becomes less characteristic, and clinically is seen to be in the typhoid state.”
Leading Indications:
- Severe cases where “blood-poisoning” is marked: ‘low’ fevers, where blood-destruction or haemolysis is conspicuous, conditions called typhus-like (typhoid), or septic after parturition or autopsy wounds. Such conditions occur late in many fevers.
- Milder cases, where vascular erethism is conspicuous-palpitation, hot flushes, sleeplessness. Such a state is frequent at the menopause or after arrest of physiological discharges or the sudden arrest of pathological discharges, and relieved by the restoration of them. Shock may cause such a state.
- Though sensitive to either extremes of temperature, cases requiring Lachesis are chiefly noted for intolerance of hot weather, hot rooms, etc., especially of direct rays of the sun.
- Local symptoms are frequently left-sided or move from left to right.
- Sleep is not easily wooed; when it comes it is restless and the patient usually wakes worse in every respect, so that he fears to go to sleep.
- The mental state varies… Incoherence, degenerating to muttering delerium in fevers, is characteristic.
- Over-sensitiveness to surface contact (touch), and to constrictions, or even to clothing which is not too tight (neck, abdomen, etc.)
- A bluish hue around wounds, ulcers, etc. from blood pigment, or venous stasis.
- Difficulty of swallowing, especially fluids, regurgitation through the nostrils.
- Onset of discharges tends to relieve most symptoms.
- Craving for alcohol, even in teetotallers.
- Bleeding in many parts, blood dark and thin; ecchymoses.
- The type of patient most susceptible to the influence of Lachesis as a homoeopathic remedy is a thin, melancholy, indolent person, changed physically and temperamentally by illness.
Aggravation: After sleep; extremes of temperature; constriction; contact; acids; alcohol; spring & summer; empty swallowing; hot drinks; motion; stooping or lying; morning; emotions; lying on left side (palpitation).
Amelioration: From onset of discharges.(32)
Causation: Injuries. Punctured wounds. Poisoned wounds. Vexation. Anger. Jealousy. Alcohol. Sun.
(33)
MATERIA MEDICA for Remedies at Similar or Earlier Stages of Disease Process
The following remedies will be given in less detail than above but will show greater characteristic features for the purposes of differential diagnosis in other stages of the disease process which may or may not result in development of N.F.
ARSENICUM ALBUM
Source: The white oxide of Metallic Arsenic. (As2 O3.) Solution and trituration.
Therapeutics:
Arsenicum is such a universally acting substance, attacking, as it does, nearly every organ and tissue of the body, that it is necessary to be acquainted with the general characteristics that will reveal it as the simillimum in any given case.
- Tendency to rapidly proceed to a condition of malignancy, ie., diseases assume a grave form, to the destruction of tissue, to a general lowering of the vital forces, and haemolysis, ending, if not checked, in death.
- Another characteristic is prostration, a prostration that is out of proportion to the severity of the complaint. The patient is exhausted after the slightest exertion.
- Nevertheless, they are extremely restless. Restless with the pains, must walk about, which helps. Also mental restlessness, feels impelled to move and when too prostrate wants others to move them from bed to bed or room to room.
- Pains have a burning character where-ever situated in the body and there is often a sensation of hot fluid coursing through the veins.
- The patient is generally chilly, despite the burning pains.
- Periodicity is a feature of Arsenicum. It occurs every other day, every fourth, seventh, or fourteenth day: the more chronic the complaint the longer the cycle.
- Putridity of discharges. This is an accompaniment of its ulcerations whether internal or external, and of the tendency of its ulcerations to go on to necrosis and its inflammations to become gangrenous.
- Allied with this is Inflammed and ulcerated parts bleed readily. Haemmorrhages occur from the lungs, bowels, kidneys and uterus.
Aggravation: From cold, midnight and after, 3am., lying with head low, exertion, after food and drink especially if cold.
Amelioration: From warmth, movement.(34)
MERCURIUS SOLUBILIS/ VIVUS
Source: I) Also known as Mercurius Oxydulatus Niger from its black colour, was the ammonium nitrate salt of mercury introduced by Hahnemann into medicine in 1788. 2(NH2Hg2)NO3H2O. It was prepared by precipitating Mercury from its solution in nitric acid by means of caustic ammonia. Trituration. Mercurius Vivus. Hg. Hydrargyrum. Argentum vivum. Metallic Mercury. Quicksilver. Although Hahnemann proved MercuriusSol., he recommended the use of triturations of the pure metal in practice as being the simplest mercurial preparation, and more easily obtained and equally available with Mercurius Sol. for prescribing on the symptoms of the latter. Trituration. (35)
Therapeutics:
A feature of Mercurius is very easy exhaustion after quite slight exertion. There is a tendency to emaciation and paretic weakness, associated with a liability to fainting attacks or sudden myocardial failure. Blood dyscrasias occur, resulting in profound anaemia which renders the subject liable to ready suppuration, characterised by sanious pus or necrotic ulceration. (36)
Leading Indications.
- Cachexia, anaemia, exhaustion, emaciation.
- Salivation; stomatitis.
- Increase and alteration of secretions, which become thin and excoriate.
- Ulceration of skin and mucous membranes.
- Perspirations which do not relieve and are foul-smelling.
- Thirst, with moisture of mouth and tongue.
- Aggravation of all symptoms at night and from warmth of the bed.
- Moist eczema and intetrigo.
- Nocturnal bone pains.
- Low-grade suppurations, which are acrid and blood-stained.
- Tremors of course character that tend to become convulsive.
- Green, bloody or mucous stools with tenesmus, “a cannot get done feeling.”
- Foul body smell.
- Mercurial symptoms occurring in syphilis.
- Catarrhs of mucous membranes, with increased mucous.
Aggravations: From both heat & cold, warmth of bed, at night, draughts, bending forwards, after eating, lying on right side, touch & pressure, motion & exertion, sweet food, lamplight & firelight.
Ameliorations: From rest, weeping, coitus. (37)
APIS MELLIFICA
Source: The honey bee is the source of this remedy, the whole insect being used in the preparation of the mother tincture or dilutions of the poison with alcohol.
Pharmacology: The chemical composition of the bee venom remains obscure, although various fractions, such as histamine, hyaluronidase and a bradykinin have been identified. It is said to be a toxalbumin, and its effects are similar to those of other animal poisons, such as the toxalbumins of the snakes, spiders, lizards, etc. Bee venom is known to have haemolytic, haemorrhagic and neurotoxic effects in addition to its profound histamine activity.
In addition to haemolysis, coagulation of fibrinogen and increased permeability of capillaries, there is also a lowering of surface tension and membranes potential, which results in reduction of osmotic pressure and facilitates diffusion of fluids, leading to oedema and effusion.(38)
Leading Indications:
- Aggravation from heat in any form.
- Over-sensitiveness: of skin, of mind, of organs.
- Sadness, indifference, suspicion, jealousy.
- Foolish or childish behaviour.
- Stinging, burning pains, with rapid change of site.
- Violence and rapidity of complaints.
- Right-sided; symptoms go from right to left.
- Absence of thirst where it is expected, ie., during heat, and also generally.
- Tight, constrictive sensations: in throat, larynx, chest, abdomen.
- Inflammation and oedema: of skin, mucous membranes, serous membranes, synovial membranes, subcutaneous tissues.
- Urticaria and erysipelas.
- Cerebral affections, especially in children; meningitis, cri cerebral.
- Morning diarrhoea.
- Prostration; faintness.
Aggravation: From heat; close rooms; from touch & pressure; in the morning; 3pm (chills); evening; night; lying down; radiant heat, getting wet.
Amelioration: From cold; cold washing; expectoration; sitting; changing position. (39)
ARNICA
Source: Arnica montana is a member of the Compositae family. It is known as Leopard’s bane, fall herb, Panacea Lapsorum. The mother tincture is prepared from root, flowers and leaves after removal of the larvae of the Arnica fly, which are commonly found on the plant.(40)
Therapeutics: It is especially suited to case when any injury, however remote seems to have caused the present trouble. After traumatic injuries, overuse of any organ, strains. Arnica is disposed to cerebral congestion. It acts best in plethora, in debilitation with impoverished blood, cardiac dropsy with dyspnoea. A muscular tonic. Traumatism of grief, or remorse. Influenza. Limbs and body ache as if beaten; joints as if sprained. Bed feels too hard. Sore, lame, bruised feeling.
Marked effect on the blood. Affects the venous system inducing stasis. Thrombosis. Haematocele. Ecchymoses and haemorrhages. Relaxed blood vessels, black and blue spots. Tendency to haemorrhage and low-fever states. Tendency to tissue degeneration, septic conditions, abscesses that do not mature. (41)
If the malady advances more definite stupor develops, and though when roused the patient begins to answer a question correctly, he lapses in the middle of a sentence into muttering delerium or unconsciousness. When a patient has arrived at this mental state he is well on in a typhus, enteric, malignant malaria, yellow fever, or sepsis (surgical, peurperal or other). The concomitants in the shape of muttering delerium, fever, rapid, weak pulse, dusky skin, possibly with ecchymoses, or congestive patches, dry tongue, sordes etc. some or all of these will now be present. (42). Prophylactic of pus infection. (Shroyens, Synthesis, Edit.5.2., Pg. 1790)
Aggravation: Walking; going upstairs; movement; spinal pain; wrist pain; various pains are worse for inspiration.
Amelioration: Movement. (Sore feeling from lying on one part, but the relief is only temporary.)
PHOSPHORUS
Source: The homoeopathic preparations were made from phosphorus obtained from bone ash. This was the yellow toxic variety, which may also be obtained from the mineral apatite, from animal bones and from basic slag, a by-product of steel-making. Potencies are prepared from a saturated solution of the yellow phosphorus in alcohol. (43)
Therapeutics: In typhoid-like conditions Phorphorus is recognisable by:
Abdomen distension; sore, very sensitive to touch. Stools offensive, bloody, involuntary. The anus appears to remain open. Worse lying on left side: better right. Burning in stomach: burning thirst for cold water. Desire for ice cream.
Fear alone; in dark; of thunder. Suspicious.(44)
SILICA
Source: Silicea terra. Pure Flint. Silex. Silicic anhydride. Silicon dioxide.(Si O2). Trituration of pure, precipitated Silica.
Therapeutics: Skin: Lymphatic swellings and abscesses, even with fistulous ulcers.-Engorgement, induration and suppuration of glands.-Abscesses which do not break, but burrow under the skin; exanthemata in general which corrode and spread. Ulcers in general; wherever pus is discharged from any part of the body; ulcers burning, scabby; indolent; when circumscribed with redness; very high, hard ulcers; with proud flesh; with corroding pus; smell very offensive. Inflammation, softening(swelling), and ulceration of bones. Mild and malignant suppurations, esp. in membranous parts. Small wounds heal with difficulty, and suppurate profusely. Mental & Emotional: weak, nervous, easily irritated, faint-hearted; yielding, giving up disposition, “grit all gone.”
Aggravation: From cold or draft, motion, open air, at new moon.
Amelioration: In a warm room, wrapping up head, magnetism and electricity. (45)
BELLADONNA
Source: The plant Atropa belladonna. It is the common deadly nightshade, a member of the Solanaceae family. For preparation of the mother tincture the whole plant is used, gathered at the commencement of flowering. (46)
Therapeutics:
Leading Indications
- Congestions and inflammations of a violent and intense character.
- Pains and symptoms come and go suddenly and are violent.
- Tendency to delerium of an active and violent kind: hallucinations, fears of imaginary things (“a black dog”) with desire to escape.
- Tendency to twitchings, jerkings and convulsions.
- Burning fever and rapid pulse, which is strong and bounding; early stages of inflammations.
- Dryness and heat of the skin and mucous membranes.
- Hypersensitivity to all impressions, drafts, noises, pressure etc.
- Great thirst not relieved by drinking.
- Aggravation of symptoms in the afternoon (3pm) and till after midnight.
- Predominance of affections on the right side.
- Symptoms are worse in the horizontal position (especially the head).
- Tendency to rapid formation of pus in external inflammations. (47)
CARBO VEGETABILIS
Source: Vegetable charcoal. It is generally made from poplar, beech or birch wood, and raised to the third potency by trituration.
Pathogenesis: Charcoal has the property of absorbing gases in its interstices, and thus ordinarily contains quantities of oxygen which, when the charcoal is brought into contact with decomposing organic matter, is released, and oxidises the putrefying mass, while at the same time the charcoal adsorbs the gases that are formed by the oxidising process. It has no direct action on the microbes of putrefaction, but favours the development of the aerobic organism at the expense of the anaerobic.
Therapeutics
Leading Indications:
- Desire to be fanned rapidly in stomach and respiratory complaints.
- Burning internally, cold externally; burning characterizes many of the Carbo-veg.
- Surface cold; dusky blue nails; dilated capillaries and veins, cold sweat. Numbness of parts lain on.
- Haemorrhages, passive oozing of dark thin blood.
- States of collapse, surgical shock.
- Septic conditions, putrid discharges.
- Conditions where there is a lack of reaction.
- Low states of vitality with venous engorgement.
- Fever: tertian type, beginning 9 to 10am. Thirst in cold stage, none in hot.
Aggravation: From hot, damp air; evening; warmth; brandy & wine, butter, pork, rich food, abuse of quinine and mercury; morning on waking.
Amelioration: From eructations, warm covering, being fanned. (48)
POTENCY
Is defined as: “The especially produced capability in a medicine to effect a dynamic stimulus in the appropriate patient (and)… is the stage of remedial activity to which a drug has been taken by means of a measured process of deconcentration, with succussion, or by trituration, of the medicinal substance, which is thus brought to a state of diminutive or infinitesimal subdivision.” (49)
Extensive investigative studies of recorded pathogenetic experiments were carried out by Henri Voisin (50) to assess the time passed before particular reactions happened in provers and also to confirm what had already been established by clinical usage. His results were that, in general:
- Low potencies are best suited to organic disease;
- Medium potencies are most effective for influencing function;
- High potencies produce the best response in mental & emotional symptoms.
For our purposes in this review, it is sufficient to assert that it has become accepted practice that lower potencies are often given in repeated doses when prescribing on the basis of morbid anatomy (as recommended by Richard Hughes, 1836-1902), and in some acute diseases provided there is no irreversible tissue destruction. But it should also be remembered that a remedy, if well indicated in terms of the law of similars, would be homoeopathic even without recourse to a potency thereof, as exemplified by the occasional use of mother tinctures, whenever one of these happens to be the most appropriate form of the remedy for the particular case.
Guidance to appropriate potencies are given in books cited in the Reference Section which are marked with an asterisk *
DISCUSSION
Based on the information reviewed concerning both the accepted theory and practice of treatment of the disease process, which can result in states of inflammation, suppuration, gangrene or necrosis as a consequence of puncture wounds (caused by drug injection), repeated over time or infected by an exogenous pathogen in those with a compromised immune system (C.I.S.), and with theory and practice in homoeopathy for treatment of similar states with similar causes, it would seem more than plausible to conclude that homoeopathic treatment is a viable alternative when antibiotics are proving ineffective, as has been the case in some instances, (51), when N.F is rapidly developing, or as a complement to such treatment as debridement and surgery when required, (especially Carbo-veg. in relation to Hyperbaric Oxygen Therapy).
Treatment using homoeopathic medicines is also highly effective in earlier stages of the disease process, which may help prevent the potential development of suppuration or sepsis at either local sites or its more serious effects when toxins have entered the bloodstream. The author has considered some of the reasons, which contribute to a lowered state of immunity. Homoeopathic philosophy has also been included, which provides an added perspective to the subject of predisposition in this particular disease manifestation, by identifying an innate pattern, which may be found to provide clues as to why these particular individuals succumbed to severe infection requiring surgery or consequently died, rather than many others in the same or similar circumstances.
Without exact figures as to the number of people who were of homeless status amongst those affected by the cited outbreaks, it is impossible to conclude just how influential this status would be to the potential rapid development of septic states, although it is clear they would be considered to be at greater risk for the reasons outlined above. Nevertheless, the author feels this is an important question for both the self-care of intravenous drug users who are also homeless but also for health-care and housing providers. Furthermore, the aim of this review has been realised, in that, six main remedies have been identified as being appropriate for treatment of the afore-mentioned stages of this disease process from inflammation through to necrosis and a resume of these medicines has been provided with additional notes regarding appropriate choice of potency if prescription of same should be considered. Originally undertaken around and completed on 18th September 2001.
BIBLIOGRAPHY
Hahnemann, S. ‘The Chronic Diseases, (Theoretical Part)’,B.Jain Pub. Ltd. Reprint Edit. 1993.
Ortega, P.S. ‘Notes on the Miasms’ 1st English Edit., National Homoeopathic Pharmacy. 1980
REFERENCES
- SCIEH, Vol..34, No.2000/24, 20th June 2000.
- The Big Issue, No.323, July 19-25th, 2001. Pg. 6-7.
- Journal of Wound Care, June, Vol.7, No.6. 1998. Pg.306.
- Fournier, A.J. Gangrene foudroyante de la verge, Semaine Medicale (Paris) 1883; 3: 345.
- Meleney, F.L. Haemolytic streptococcus gangrene, JAMA 1929: 24, 2009-2012.
- Bakker, D.J. Selected aerobic & anaerobic soft tissue infections: diagnosis & the use of HBO as an adjunct. In: Kindwall, E.P. (ed) Hyperbaric Medicine Practice, Flagstaff, A2: Best Pub. Co. 1994.
- Journal of Wound Care, January, Vol.8, No.1. 1999; Pg. 18-19.
- Ibid.
- Ibid.
- Scanlon & Saunders, Essentials of Anatomy & Physiology, 2nd. Edit. 1995, F.A Davis & Co. Pg.403b.
- Ibid. Pg.405b.
- Youngson, R.M. Dictionary of Medicine, 1999. Unwin & Hyman Pub.
- GGHB News Update, 30th May, 2000. Pg.1.
- Frobister & Fuerst, Microbiology in Health & Disease. (Philadelphia: WB Saunders, 1973, Pg.192-3.
- Fisher, R.B. & Christie, G.A. A Dictionary of Drugs, 2nd Edit. Paladin, 1982.
- Journal of Wound Care. January, Vol.8, No.1. 1999, Pg.18-19.
- GGHB News Update, June 15th, 2000.
- Frobister & Fuerst, Microbiology in Health & Disease. (Philadelphia: WB Saunders, 1973. Pg.168.
- Shaw, B. The Doctors Dilemma.
- GGHB News Update, 30th May 2000, Pg.1 of 3.
- GGHB News Update, 15th June, 2000, Pg.2 of 3.
- Tortora,Funke & Case, Microbiology; An Introduction. 5th Edit. 1994. Benjamin & Cummings Pub.Co.Pg.369t.
- GGHB News Update, 15th June 2000, Pg.1 of 3.
- Frobister& fuerst,Micribiology in Health & Disease, (Philadelphia, WB Saunders, 1973. Pg.276.
- Vithoulkas G. The Science of Homoeopathy. 1992, Pg.78. B. Jain Pub.Co.
- Gaier, H. Thorsons Encyclopaedia of Homoeopathy, 1991. Thorsons Publishers Ltd.
- GGHB News Update, 19th May 2000. Pg.1 of 1.
- Gaier, H. Thorsons encyclopaedia of Homoeopathy, 1991. Thorsons Publishers Ltd.
- Ibid.
- * Neatby, EA & Stoneham, TG, Manual of Homoeo-Therapeutics. Reprint Edit. 1989 B. Jain Pub. Ltd.
- *Gibson, D. Studies of Homoeopathic Remedies. 4th Reprint Edit. 1996 Beaconsfield Pub.
- Neatby & Stoneham
- *Clarke, JH. A Dictionary of Practical Materia Medica, Vol.II. 1994. Reprint. B.Jain Pub.Ltd
- Neatby & Stoneham.
- Clarke, JH. A practical Dict. Of M.M. Vol II. Reprint 1994.
- Gibson, D. Studies of Hom.Rxs. 4th Reprint 1996.
- Neatby & Stoneham
- Gibson, D.
- Neatby & Stoneham
- Gibson, d.
- Neatby & Stoneham
- *Boericke, W. Pocket Manual of Homoeopathic Materia Medica, Reprint Edit. 1994, B. Jain Pub. Ltd.
- Neatby & Stoneham
- Tyler, M. Pointers to he Common Remedies, Reprint Edit. 1995, B. Jain Pub. Ltd.
- Clarke, JH. A Dict. Of Practical M.M. Vol. III, Reprint Edit. 1994. B.Jain Pub. Ltd.
- Gibson, D.
- Neatby & Stoneham.
- Ibid.
- Gaier, H. Thorsons Encyclop. Of Homoeopathy, 1991. Thorsons Publishers.
- Voisin, H. Die vernunftige kritische Anwendung der Homoopathie, translated and Pub. By Fritz Stockerbrand,1960.
- GGHB News Update. 15th June 2000, Pg. 2 of 3.

Brilliant articele, Jacqueine. So well researched and beautifully classical.
Ingrid
Thanks Ingrid. The Ebola situation and possibilities for homeopathic treatment reminded me of this previous research for the genus epidemicus, I’d completed. And of course, because of haemorraghic symptoms similar remedies do appear.
Stay well. X
Did you consider the brown recluse spider? The bite causes a similar non-healing wound. I dont have the remedy name easily at hand.
Lox-recl