

Preliminary Data: Female, 45 years, married, middle class
Acute history
A 45 year old lady arrived in the ER of a general hospital in an unconscious state on 25.9.98. The RMO on duty took the following history:
She was found on the floor at home deeply comatose at 2.30 pm today. No spontaneous movement in any limbs, not responding to call. No vomitus was seen and no convulsions were observed. She has no other significant history, except for complaint of a headache last evening.
She was in apparent good health until 10 am in the morning when her husband and son left for work. She was alone at home when this occurred and was found unconscious at 2.30 pm by her son. There was no other eye witness account. She was a known case of hypertension and had developed hyperthyroidism over the last 4 years. Earlier she was on allopathic treatment but had stopped it in favour of Aayurvedic treatment.
It was obviously an inadequate history from the homeopathic point of view, as all available data was from the allopathic RMO.
2. Examination
On admission; 25.9.98
Deeply comatose
PR: 95/min
BP: 190/110
Chest, CVS: NAD
PA: soft
CNS: Eyeballs deviated downwards; Dolls eye movement absent
Pupils small but reacting, Cranial nerves ?
All 4 limbs limp, quickens only on painful stimuli
DTR: N; Brabinski’s positive; No meningeal signs
Impression: CVA with brainstem haemorrhage (Homeopathy for Haemorrhage)
3. Investigations
25.9.98 (from the Emergency Room)
HB; 13.3; WBC 18,800; N81, L19; ESR 25; RBS 151
Na 142, K 3.5; Cl 104; CO3 22; Urea 24; Creat 0.8; Calcium 9.6
LFT: Bil 0.5; Prot: 7.3 Alb 4.2 Glob 3.1 SGOT 6 SGPT 108 PT 12
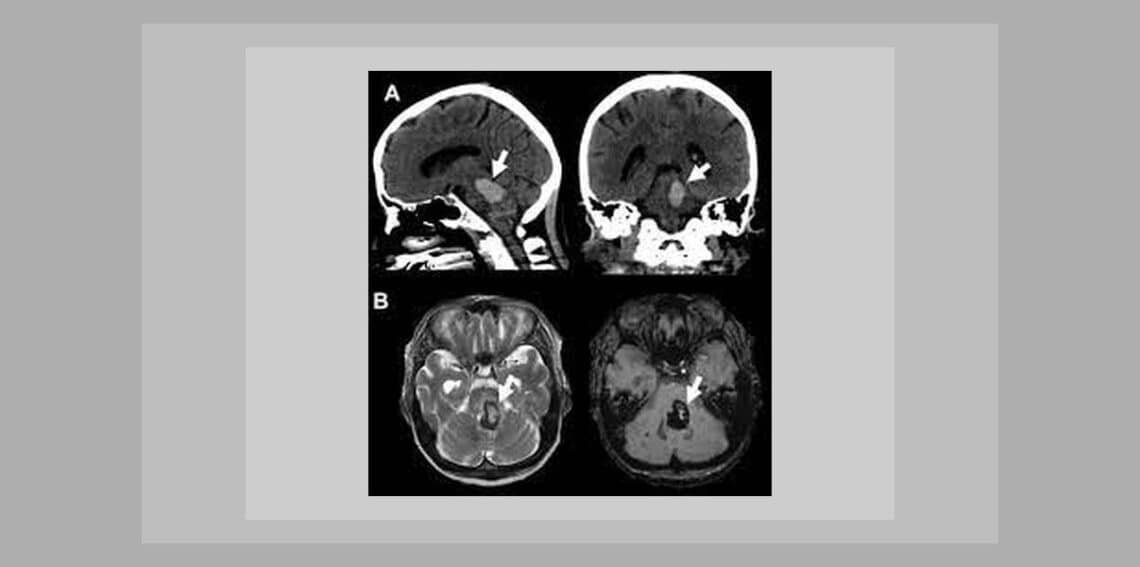
CT Scan: (ref: Annexure DC 2A)
4th ventricle is compressed. Diffuse, large abnormal area of increased density is seen in the pons with surrounding hypodense edema. The attenuation values are in the range of clotted blood. The surrounding basal cisterns are effaced.
Ct appearances are those of pontine and brain stem hemorrhage.
4. Diagnosis:
Known case of hypertension and hyperthyroidism, with brainstem, pontine hemorrhage in coma.
5. Emergency Analysis and Totality:
Since the patient was seen by me only 17 days after the actual emergency presentation, the analysis of the retrospective history could only be made on the investigations and diagnosis. The follow up notes explained that she had developed a lot of secretions and wheezing on admission.
Whether this was related to the acute CVA or whether it was a result of aspiration due to the comatose state is difficult to tell. Allopathic emergency treatment was aimed at controlling the blood pressure, reducing brain edema and hopefully assisting the clot absorption. Along with this, nebulizer with steroid and suction were given for the respiratory symptoms.
The acute totality of the pathology:
o Internal bleeding and clot in the brain
o Edema of the brain following injury to blood vessels (CVA)
o High blood pressure
o Unconsciouness
The rubrics from Complete Repertory
o Mind; UNCONSCIOUSNESS, coma; General; brain complaints, in (m, 34, 1-1)
o Head; HEMORRHAGE, brain (p, 68, 4-4)
o Clinical; HYPERTENSION (p, 131, 5-6)
o Generalities; WOUNDS; Swollen (p, 13)
Arnica, Bellis-p, Puls, Aconite, Sulph were the remedies covering all these rubrics.
The obvious choice for a cerebrovascular accident from the pathological standpoint is Arnica.
When I saw the patient in the ICU, there was also a mild respiratory distress, probably due to aspiration? Removing the profuse secretions by suction seems the only way to relieve her, as she could not remove them herself being unconscious.
From the Universale V Repertory
o Respiration; M; MUCUS, from accumulation of (m, 46)
o Respiration; P; DIFFICULT; Expectoration; amel. (m, 22)
o Mind; P; UNCONSCIOUSNESS, coma; General (p, 400, 388-1636)
Antim Tart as a specific was the obvious choice to help alleviate the respiratory problem, though the other remedies were Phos, Ipecac, Zincum.
6. Chronic History:
The history was obtained from her husband. The highlights were:
She is a very responsible person who took on the responsibility of the home and her son completely. She is very keen that her son settles down with a good job position. Her husband is a civil servant with the government and is always traveling due to his work.
She is fastidious and likes to keep the home very neat and clean. Yet she is a very kind person, fond of animals and enjoyed music and dancing. Besides this high sense of responsibility, there was nothing else that troubled her.
She is always the one to help other members of the family. She suffered from hypertension for the last 5-6 years and was on antihypertensives which she stopped when she started Ayruveda. She was had hyperthyroid and was given treatment earlier on, but had decided to take only Ayurvedic medicine for this.
She seemed to be doing well on that treatment and suddenly this occurred. There was a family history of cancer and diabetes. She likes fruits and juices and was vegetarian. She had scanty perspiration and nothing remarkable in terms of bladder and bowel habits. She is ambithermal.
The rubrics used from Complete repertory were:
o Mind; RESPONSIBILITY; Strong, too (p, 36, 5-8)
o Mind; FASTIDIOUS (p, 75, 3-11)
o Mind; DANCING; Desire for: acon., aether, Agaricus, agath-a., aids, amet., ana-i., androc., apis, apisin., arist-cl., Belladonna, bos-s., bros-g., calc-p., camph., cann-i., cann-s., caras., CARC., chir-f., chlol., Cicuta, clad-r., Cocc., con., Croc., croto-t., fl-ac., grat., Hyoscyamus, ign., kola., lach., lat-h., loxo-r., lsd, mate, merc., nat-m., nitro-o., onc-t., ozone, ph-ac., pip-m., Platina, posit., rob., salx-f., sant., sep., sil., stict., Stramonium, tab., TARENT., tax., teg-a., uran., verat.
o Mind; LOVE; Animals, for (p, 20, 5-6)
The two prominent remedies are Carc and Nat Mur. Carc was chosen because of her care and concern for the rest of the family, her tendency to take on a lot of responsibly and her food desires. The family history of cancer also played a part in this decision. It is possible she would need Natrum mur in the future if components of that remedy came up. Hypertension (salt imbalance) would also indicate that remedy.
7. Plan of Emergency Management (homeopathic)
Since I had seen her much after the real emergency, it was not possible to elicit emergency signs and make observations that would indicate an acute prescription. The focus was now on dealing with the prominent pathology.
There were two pathologies presenting – one was the brain haemorrhage into the pontine area that showed clotted blood on CT scan, along with edema of the surrounding brain tissue, precipitating in coma.
The second was the respiratory distress with excessive secretions that needed to be suctioned regularly. This too may have been due to aspiration and have a different causative factor, but it was not a result of chronic problems.
I decided to prescribe two separate acute remedies for this first while the chronic remedy was being evaluated. This would result in symptomatic relief first, which was the immediate need as 17 days on allopathic treatment had not changed anything (the Neurologist giving a very poor prognosis (9.10.98).
The homeopathic plan, hence, was to start acute remedies at frequent dosing in low to moderate potency, aiming mainly at the pathological symptoms. This would be continued as long as the pathological symptoms had not yet resolved.
It’s important to note that allopathic management continued alongside the homeopathy . Since this is essentially symptomatic management, drugs are reduced or changed based on the symptomatic change observed.
A positive response to homeopathic treatment would result in some drugs being discontinued. Standard allopathic protocols for emergency management of CVA continued as indicated however, along with the homeopathic remedies.
8. Plan of Chronic Management
Once the acute treatment had begun to have an effect, the constitutional remedy was added as the basic stimulation towards cure. Initially, infrequent doses would be given to ascertain the response of the vital force and then symptoms were re-evaluated. Based on this, the frequency of repetition would be decided.
Opinions from experts, such as the neurologist and MD physician are important in deciding changes in treatment, or introduction of intercurrent remedies when required. Following 16 days of status quo, the first neurological opinion before homeopathic treatment was “poor prognosis” on 9.10.98, which was changed to “good prognosis” on 15.10.98, just 6 days later, and finally “good recovery” on 15.11.98.
At one point there was an infection following the tracheostomy tube insertion, and repeated courses of antibiotics had proved to be useless. A referral was made to me by the MD Physician for a homeopathic remedy instead. A specific remedy was needed to control the discharge and infection. The indicated homeopathic remedy, Silica, removed these symptoms in 3 doses of 200C (see 26/10 – 4/11).
Another intercurrent was indicated when she became very emotional with weeping due to regular dyspnoeic episodes she was having for a week or so. She did not want to be left alone and wanted to go home. Three doses of Pulsatilla 200C (7.12.98) helped her to settle down, though the dyspnoeic episodes continued.
In another instance, physostigma was given as intercurrent for visual problems and was quickly stopped in case it had contributed to the sudden bouts of obstructed breathing (see 3/12 – 5/12).
9. Ancillary Measures
Various ancillary measures are indicated in a comatose patient:
Intubation for oxygenation and controlled ventilation
IV fluids for hydration
Ryles’ tube for nutrition
Urinary catheter insertion to manage and measure urinary output
Tracheostomy if there are breathing problems
Once consciousness was regained:
General Physiotherapy
Regular Exercises
10. Follow Up
28.9.98
Brainstem haemorrhage GC same; Comatose, not responding to stimulus; not moving the limbs; put on ventilators.
RX: Amdepin, Tenormin, Nimodip, Ampicillin, Mannitol, Depin 10Mg SOS
29.9.98 : Hb 14; WBC 29600 L7, E1, N91
3.10.98 : CT Scan: The pontine haemorrhage has partially resolved to 17X21 mm. Mild prominence of ventricular system remains unchanged. No fresh bleed.
9.10.98: (Neurologist Opinion)
Patient’s condition the same. Eye opening nill, Pupils both NS, reacting to light, Hypotonia all limbs; Motor response nill; Plantars Up
Throat secretions ++ Adv: tracehostomy as patient will be unconscious for a very long period. Overall prognosis poor.
8.10.98 : Chol 205, Tgl 174; LDL 120; VLDL 29
WBC 17300 L23 N75 Hb 11.5; Urea 36
12.10.98:
A referral for homeopathic treatment was sent to me 17 days after admission. I saw the patient for the first time in the ICU on a ventilator. The patient was in coma and obviously unable to answer any questions. Observations were made and a history was obtained from the nurses on duty. She was breathing heavily and suction was being done regularly. My notes in the IPD case sheet were recorded as follows:
History noted. Diagnosis of pontine bleed, now in coma.
H/O Headache the evening previous to CVA probably indicative of increased blood pressure, otherwise nothing eventful noted.
Would like to meet the relatives in the OPD tomorrow for complete chronic history.
OE – Harsh BS with wheezing; profuse secretions +++.
CT scan: Pontine bleed with clotted blood and edema of surrounding tissue.
Adv: Arnica 30 3 pills tds; Antim tart 200 III doses
13.10.98: Complete homeopathic history taken from relatives (see chronic history);
Adv. Carcinocin 200C III doses HS x 3 days (13/10,14/10,15/10); Antim Tart 200C OD x 2 days; Arnica 30C 3 pills tds
15.10.07: Chest clear; Patient responding to pain, withdrawing the legs. There is improvement in the general condition probably due to the resolving clot in the pontine region and reduction in surrounding edema. The Arnica and Antim Tart as acute specific remedies have helped. However, due to the late stage intervention, a constitutional remedy is required.
Rx: Carcinosin 200 tonight one dose; Arnica 30 tds
15.10.98: (Reviewed opinion of Neurologist)
Comatose patient. No response to deep pain, but easily withdraws legs to plantar stimulation. Plantars partially responding.
Impr: pontine haemorrhage – prognosis is good.
17.10.98: Improvement noted by neurologist. Good prognosis has followed quick response to constitutional remedy. Since improvement remains status quo, more stimulus is required. Adv: Carcinocin 200, on 17/10,18/10,19/10
20.10.98: Better. Patient now is opening her eyes to call. BP has stabilized to average 130/80 from 160/100 earlier. Regular dosing of constitutional remedy is helpful. Rx: Carcinosin 200 3 pills HS; Arnica 30 3 pills tds
30.10.98: (MD physician) Pus discharge and infection not responding to antibiotics given. Secretions continue. Air escaping from around the tracheostomy tube. Refer for homeopathic opinion. Add Inj: Cephatoxime.
2.11.98: Yellow pus discharge from tracheostomy site not resolving. Chronic infection present. Pus, non-offensive. Specific intercurrent remedy for chronic pus indicated. Rx: Carcinosin 200 HS, Arnica 30 bd; Silica 200 III doses 12 hourly
4.11.98 (MD physician) Better, needs physiotherapy regularly. No pus from tracheostomy site. Change tracheostomy tube. Discontinue cefatomine
4.11.98: Secretions much less. Complaints of pain in the the knee joints yesterday. CT Scan – complete resolution of pontine haemorrhage (Ref Annexure DC 2B)
Rx: Carcinosin HS, Arnica 30 OD daily morning.
10.11.98: Much better, conscious, answers questions. Will taper off dosing. Rx: Discharge on: Carcinosin 200HS; Arnica 30C alternate day.
11.12.98 (Neurologist)
Patient has made a “good recovery“. Conscious, following commands, moves all the limbs; right more than left; Planters: Babinski’s positive.
Pt. was discharged on Carc 200C alternate day; Arnica 30C alternate day.
Discussion DC1
(Ref Annexure DC 1C for Case Summary)
This present case is an example of homeopathic management in an allopathic institution. Allopathic management in terms of ancillary meansures, nebulizers, IV fluids, investigations, procedures, drugs like antibiotics, steroids, were continued alongside the homeopathic treatment.
This did not interfere with the homeoapthic treatment and homeopathic indications for remedies were clear and unmasked. This was so obvious from the clear response to every remedy prescribed, that it even took the MD’s completely by surprise.
The course of treatment complications like the tracheal stricture, could have been avoided if the patient had regained consciousness much earlier avoiding the necessity of a tracheostomy. This would have been possible if homeopathic management was started right at the time of presentation in emergency.
Its possible that different remedies would have been indicated at that point taking into account acute characteristic signs and observations. Experience in a few more subsequent brain hemorrhages showed that Arnica is the best emergency remedy to start with, to begin the resolution of the bleed and clot, which is the main cause of edema and increased intracranial pressure leading to unconsciousness.
The constitutional remedy, when acute problems have begun to resolve, is vital in enhancing the improvement of the pathology as well as the general conditions of the patient. The neurologist was completely taken aback by the sudden turn around in the case from ‘poor prognosis’ to ‘good prognosis’ to ‘good recovery’.
The supportive and open attitude of these MD physicians was vital in making accurate interpretations of clinical response and progress on homeopathic remedies. Vital also was the close and alert observation of deterioration and clinical progress that was made by the MD physicians, which removed the burden of this evaluation from the homeopath’s shoulders.
The response of this patient to homeopathy was followed by a flurry of referrals from the ICU for homeopathic management alongside the allopathic treatment. Arnica 30, because it’s a lifesaving remedy for every admission of CVA with bleed, was administered by nursing staff on MD physicians orders, on a tds frequency as soon as the patient was admitted to the ward…. even before I arrived on the scene for an evaluation and opinion on homeopathic management!
————————————————
Dr. Leela D’Souza, MD (Hom)


Hello Doctor – My father has got a pontine brain hemorrhage .He got on april 10 2009.His recovery is slow.He was beforehand on ventilator but it is removed now.
he breathes normally, his pulse, b.p is normal but still he is in stage of semi unconsciousness not in fully coma . He opens his eye . His age is 45 . Therefore please suggest me about chances of his recovery as well as some medicines . I will be highly oblique.Please send it at my mail address
Hello doctor,
My mother, age 50, is sufferring with pontine brain stem hamorrhage. She went unconscious on 14 december 2010 and is still in same mode. Her bp was about 220/110 when admitted on 14 dec but rt now the same is under contrl and is at the range of 120-130/80.
However, she is still on ventilator and the recovery is much slw. Doctors say that she is taking intermittent breathing on her own but that is not sufficient to remove the ventilator. There is some body movement but the same may be on account of reflexes / not sufficient enough. Her condition has neither detriorated nor improved in these 84 hours (though her bp is brought under control)
Kindly suggest her chances of recovery and any specific medicine / treatment. I would be highly obliged by your comments. You can reply me on my e-mail address
My mother had a brain hemorrhage on Feb 6th, 2012 and we immediately took her to the near-by hospital; later, doctors have identified it as brain stem hemorrhage.
She was put on ventilator soon after admitted to the hospital and in the last 14 days, she literally has not shown any sign of improvement.
We had two CT Scans – one each on Feb 6th and Feb 9th, 2012 – both showed more-or-less the same issue.
She only responds to our call, and open her eyes for a moment. But other than this, there is no movement in her other body parts.
According to doctors, her other body organs (internal) are working absolutely fine – It’s just she is not able to breathe herself, which is supported by ventilator.
Her tracehostomy was done on Feb 15th, 2012 since diagnosis is expected to be a prolonged process.
I read your aforementioned article, which describes the same condition of patient as of my mother.
I was hoping if there could be some consultation from you since you have handled the similar case excellently in the past.
Hi Vipin,
I just read your mother’s case and wanted to know how she is doing now? My father is going through the same situation since the past 12 days, and so any help from your side would be appreciated. Please let me know from where she was undergoing her treatment and about her current situation.
Waiting for your reply..
Hello Doctor – My husband has got a pontine brain hemorrhage .He got on april25 2012.His recovery is slow.He was beforehand on ventilator but it is removed now.
he breathes normally, his pulse, b.p is normal but still he is in stage of semi unconsciousness not in fully coma . He opens his eye . His age is 37. Therefore please suggest me about chances of his recovery as well as some medicines . I will be highly oblique.Please send it at my mail address
Hello Doctor,
my brother in law is in same condition as Abhishek’s mother, my brother in law is 42-43 year old, he is hospitilized . he had pontine hemorrhage on 11-nov-2012. he had 2-3 cm bleeding, he is in coma right now. he can’t move his limbs and can’t open his eyes, he can’t even breath properly. he is on ventilator, Doctors are saying that they gonna put him on ventilator for next one more week. if they see that there is any recovery so they will keep him on ventilator for more time. otherwise they will switch off to the ventilator. please suggest what we have to do and suggest any medicine. email me at my email address.
thanks.
Don’t waste your time and put your patients life at risk,buy asking questions here!
You will never get any response.
Please re-read the above case.Where is Homeopathy here? Ex:- Physostiga (Pilocarpine) for visual problem. Is this the way to prescribe in homeopathy?