

Introduction
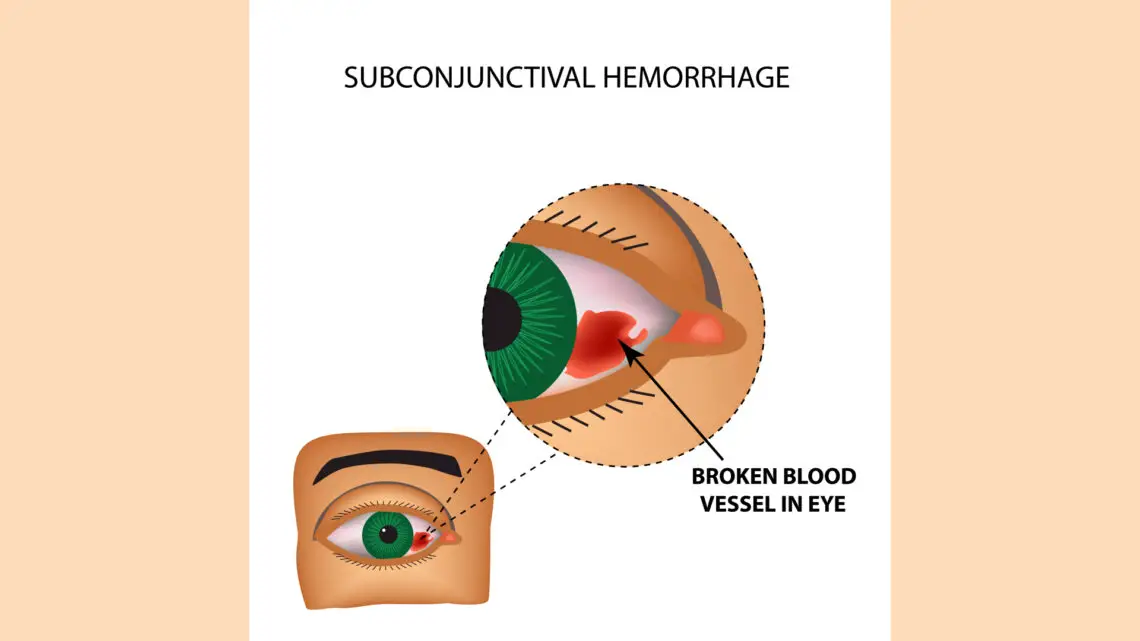
Subconjunctival haemorrhage (SCH) is considered a benign condition, most commonly presenting as circumscribed redness and bleeding underneath the conjunctiva, varying from ‘dot-blot haemorrhages’ to extensive areas of bleeding covering the entire sclera [i].
Tarlan and Kiratli i identify that among older patients SCH is mostly associated with systemic vascular disorders, including hypertension, diabetes or arteriosclerosis, whereby the walls of the blood vessels become fragile; whereas in younger patients, causes more commonly include ‘local trauma to the globe, injuries to the orbit, acute inflammation of the conjunctiva, conjunctival tumours, conjunctivochalasis, ocular amyloidosis, contact lens usage, ocular surgery, and ocular adnexal tumours’.
Accordingly, SCHs do not necessarily require specific treatment, as the haemorrhage will usually disperse by 3 weeks i. Some patients seek individualised homeopathic treatment to ensure the SCH clears up more quickly.
Furthermore, classical homeopathy can address any underlying or accompanying vascular issues [ii]. This can also be demonstrated with regards to migraines, which may be caused by vasodilatation of the cerebral and meningeal arteries, or activation of the trigemino-vascular system [iii].
In such circumstances, the whole case needs to be taken and the homeopathic remedy and potency carefully selected according to fundamental laws of homeopathy including the Law of Similars and the Law of Minimum Dose. The correct remedy may be prescribed by considering the totality of symptoms and/or using keynote symptoms.
Case study
A 43-year-old woman presented with burst blood vessels in the right eye, which was the second time she had experienced such an issue. She stated the possible causative factors for the previous occurrence 5 years ago to be very firm massage.
Preceding this second SCH, she had woken with a headache that felt like the end of a migraine (the patient suffered from migraines, an important feature of the case, outlined below), and then bent down and felt heavy in the head. She was crying and had emotional upset, and a sore back from overwork the previous evening.
Apart from the migraines, the patient was also plagued for many years with urinary tract infections (UTIs), to the point that she was prescribed to take antibiotics after any sexual intercourse. She had been less sexually active since her last partner, and even then, she only had them rarely during that relationship, so she hadn’t had a UTI for ‘a couple of years’. She also used to get styes. She felt weakness in her blood vessels. She said she ‘runs cold’, with cold feet and cold hands.
She also suffered with low blood pressure, anxiety (previous history of panic attacks, agoraphobia and derealisation/dissociative symptom of panic disorder), hay fever and varicose veins (one was severely bulging, which came up on her right leg after the birth of her first and only child 23 years prior) and she smoked cigarettes.
Besides her addiction to nicotine, she was concerned about becoming addicted, losing control, and ‘not being able to stop the physicalness’ with regards to other substances; for example, this was a concern for her when she was prescribed Valium for the panic states.
The migraines occurred every month on average (usually before her menstrual period), sometimes more, sometimes less, and the patient thought there could be a hormonal component to them. She suffered a great amount of pressure with her headaches.
She used to get migraines often, but in recent times they had become less frequent. They began after the birth of her child. They usually would last for several hours and sometimes occurred twice in a row. Occasionally, she would experience disturbed vision and vomiting.
Sometimes her eyes would ‘feel funny’ upon waking and this sensation signified the beginning of a migraine, at which point she would take 3 Panamax and lay down for a couple of hours. The pain was felt on the inside of the front of the head, behind the eye.
It was a deep pain with heaviness, aggravated by light, movement of any kind and thinking about the pain. After the migraine subsided, she would become very hungry – usually going for something like avocado on toast or a big meal like junk food as a ‘reward’ for getting through the intense experience.
Her paternal grandmother also had headaches (as well as varicose veins) and would treat them with aspirin. Other illnesses that occurred in the family included cancer, hypertension and stroke, anxiety and dementia.
The patient’s sleep in general was ‘not great’. She would go to bed between 2am and 4am and sleep in so as to obtain 7 to 8 hours of sleep: She had ‘always been a night owl’. In general, the patient preferred savoury to sweet, and desired salt on everything.
She would drink two double-shot coffees every morning. Spicy food would aggravate her urinary system. Her menstruation was very regular and would last 3 to 4 days. She sometimes could experience pre-menstrual stress (PMS).
Further mental and emotional symptoms recently included concern about finances due to being off work for 4 months because of vaccine mandates. She was stressed about her ‘reserves running out’.
The remedy selected – Medorrhinum – was initially considered based on keynote prescribing (Vithoulkas[iv]); however, we continued to confirm the remedy based on the other symptoms outlined above and upon further questioning.
For example, I asked the patient about any history of sexually transmitted infections, and she confirmed she had contracted gonorrhoea 17 years prior: It was then revealed that this infection was the precursor to her continued UTIs.
The potency of the remedy was selected based on the patient’s Level of Health, which was estimated to be in the upper levels of Group B.
Prescription: Medorrhinum 1M, one dose only.


Before the remedy:


2 days after the remedy:


4 days after the remedy:

1 week after the remedy:
2 weeks after the remedy: The patient reported that she hadn’t had a single headache since the remedy, she was feeling better overall, sleeping better, and (to her surprise) going to bed earlier.
In contrast to her last SCH, the length of time of recovery was much shorter, despite this second experience being more severe. The patient decreased her coffee intake by half.
3 months after the remedy: The patient had a ‘return of old symptoms’ in the form of a lump in her right breast. 5 years earlier, she had been diagnosed via ultrasound with ‘a few’ cysts in the deeper tissues of her breast. The cysts were previously drained using a needle. This time, it was just one lump, and it was far more superficial, and came and went without any intervention. There had been no headaches during this time.
6 months after the remedy: There had been no further problems with the patient’s eyes or blood vessels. She had not had any UTIs either and was not getting any anxiety nor hay fever. The large varicose vein on her right leg was slightly better, but the varicose veins in general were still prevalent.
She had been feeling achy and lethargic lately, yet also happy and independent. She had suffered with approximately 3 migraines, although they had been less intense, except for the last one. The last migraine came on due to stress and lack of sleep.
Upon further investigation, the patient had begun taking a ‘homeopathic’ sleep aid, consisting of multiple remedies (polypharmacy): Melatonin 6X, Nux vomica 30X, Coffea cruda 6X and Arsenicum album 30X. She bought this product after an 8-day poker tournament that had left her exhausted as she was unable to sleep enough during this time due to the excitement and absence of good routine. Two migraines occurred since then.
The over-the-counter combination remedy interfered with the original prescription. However, I needed to consider that she was having trouble with her sleep and could have potentially already been starting to relapse.
Still, the organism may very well have come back into balance after the environmental stress and excitement had passed. Certainly, since taking the ‘homeopathic’ sleep aid, the migraines were worse again. She also explained that she was starting to feel some anticipatory anxiety about taking a flight the following year as she hadn’t been on an airplane in a long time. She discovered during the most recent migraines that B12 supplementation lessened the pain, so she identified a deficiency and chose to continue supplementation.
Prescription: Repeat the Medorrhinum 1M due to antidoting, one dose only.
The patient did not take the remedy immediately as she was on holidays. In the meantime, an infection began in the outer nail bed of her left big toe. She also experienced another migraine during this time. She was advised to take the Medorrhinum 1M immediately, and after 3 days the toenail infection had completely healed.
10 days after the remedy she reported feeling ‘a niggling headache for a few days’, and increased urination ‘like at the beginning of an UTI’. Neither the migraine nor the UTI manifested, so it is understood that these ‘niggly’ sensations were mild physical aggravations following the repetition of the Medorrhinum 1M and we could expect continued amelioration of those symptoms in particular[v]. She was no longer drinking coffee and had reduced her tobacco intake as well. On the mental and emotional levels, the patient said she felt ‘calm inside’, and was overall very well.
Discussion
Though subconjunctival haemorrhage has a variety of aetiologies and is generally short-lived and self-limiting, classical homeopathy can provide faster relief as well as address potential underlying causes. In this case, an undiagnosed systemic vascular disorder may have triggered the walls of the blood vessels to become fragile. We could further speculate that this unidentified pathology may also have been the underlying instigator of, or contributing factor for, the chronic migraines.
By using individualised homeopathic prescribing, we can address issues affecting the whole person as well as more superficial symptoms such as SCH. In classical homeopathic prescribing, the correct remedy is most often selected based on the totality of symptoms; however, keynote prescribing is also extremely helpful. This is in contrast to non-classical polypharmacy, such as that found in over-the-counter ‘homeopathic’ products; which, if taken in conjunction with classical homeopathy, can interfere with the positive action of the best selected remedy.
Conclusion
In this case of subconjunctival haemorrhage, the patient benefited from individualised classical homeopathy. The benefit extended to her more chronic complaints of migraines and general wellbeing as well. Scientific investigation into the relevance of homeopathy in subconjunctival haemorrhages and vascular disorders is warranted.
[i] Tarlan, B. & Kiratli, H. 2013. Subconjunctival hemorrhage: risk factors and potential indicators. DOI: 10.2147/OPTH.S35062
[ii] Crotty, T.P. 1989. Homœopathy and homeostasis in the vascular system part 1. DOI: 10.1016/S0007-0785(89)80004-3
[iii] Biswas, R. 2018. Migraine in homeopathy: An Update. tjhms.com/uploadfiles/9-12.20181206111223.pdf
[iv] Lecture number 5 on Materia Medica, IACH E-Learning program.
[v] Vithoulkas, G. 2017. Levels of Health.


Excellent work Sarah !