

About The Disease
The most common cause of hyperandrogenism and hirsutism is PCOS. The association of amenorrhoea with bilateral polycystic ovaries first described by Stein and Leventhal in 1935 and was known for Stein Leventhal Syndrome for decades. In the past all the clinical diagnosis made on the triad of hirsutism, amenorrhoea and obesity. Later on it is researched out that PCOS has an extremely heterogenous clinical picture and is multifactorial in aetiology.
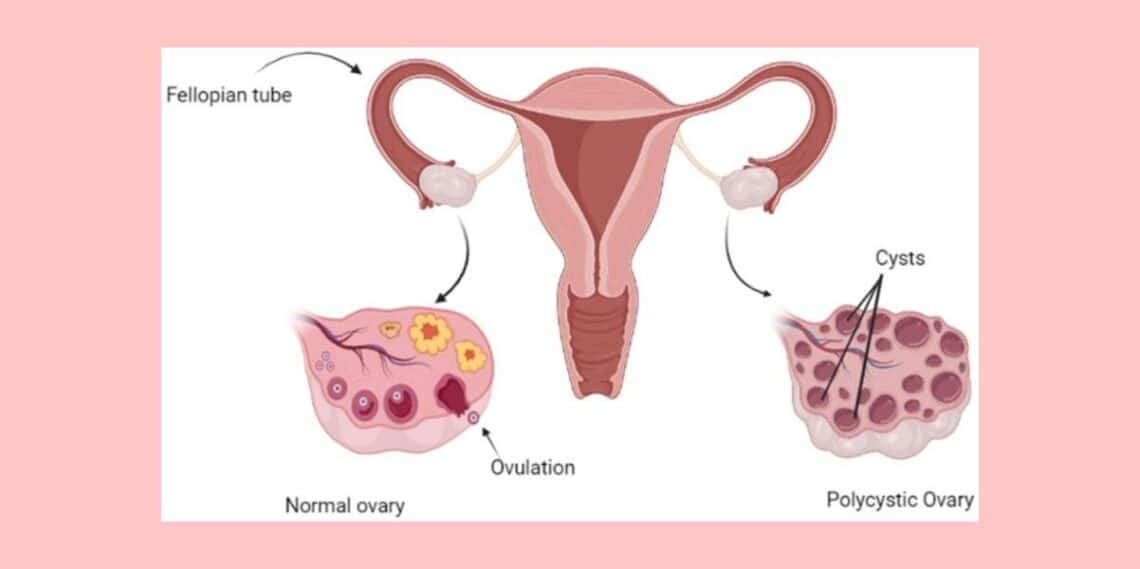
This complex disorder is characterized by excessive androgen production by the ovaries/adrenals which interferes with the growth of the ovarian follicles. Therefore PCOS is a state of androgen excess with chronic anovulation. The incidence varies between 0.5 – 4%, more common in infertile women.
Diagnostic Criteria:
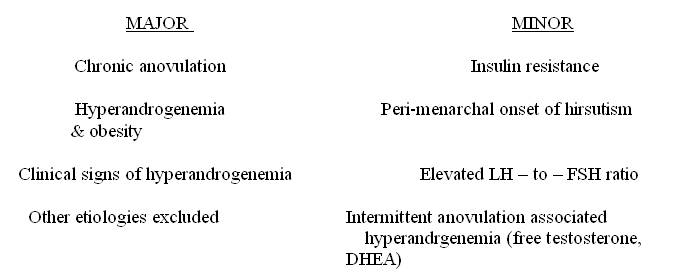
Hirsutism:
In United States it is common in 70% of the patients with PCOS whereas in Japan it is only 10 – 20%.
Menstrual Dysfunction:
Oligomenorrhoea to amenorrhoea are the common findings in PCOS. As a rule the patients of PCOS exhibit anovulation. Even in hyperandrogenic women with regular menstrual cycles, the rate of anovulation is 21%. Severe acne in teen age years appears to be a true indicator of PCOS.
Obesity:
It is found in 50% of patients with PCOS. The body fat is usually deposited centrally (android obesity) and a higher waist to hip ratio indicates an increased risk of diabetes mellitus and cardiovascular diseases. Apart from excess production of androgens, obesity is also associated with reduced SHBG (sex hormone binding globulin). It also induces insulin resistance and hyper-insulinemia which in turn increases the gonadal androgen production.
Insulin resistance and hyper-insulinemia:
These are very common in the patient of PCOS.
Abnormal lipoproteins:
Very common in PCOS and include elevated total cholesterol, Triglycerides, LDLs, low levels of HDLs and apoprotein A – I. The most important factor is decreased levels of HDL2 alpha.
Acanthosis Nigricans:
It is considered as a marker for insulin resistance in hirsute women. This is characterized by specific skin changes due to insulin resistance. The skin becomes thickened and pigmented. Nape of the neck, axilla, inner thighs are the commonly affected sites.
Hair -An Syndrome:
Women with severe insulin resistance sometimes develop this type of syndrome consisting of hyperandrogenism, insulin resistance, acanthosis nigricans.
Pathophysiology
The exact pathophysiology is not clearly understood. Several theories explain the pathophysiology:
Hypothalamic – pituitary compartment
- Increased pulse frequency of GnRH
- Increased pulse frequency of LH (Leptin, a peptide which is secreted by fat cells and ovarian follicles in presence of hyperinsulinemia may be responsible for this)
- GnRH is preferential to LH rather than FSH
- Increased pulse frequency & amplitude of LH results in tonically elevated level of LH
- FSH level is not increased due to negative feedback effect of chronically raised estogen & follicular inhibin.
- Increased free estradiol due to reduced SHBG bears positive feedback relationship to LH
- The LH : FSH is increased.
Androgen Excess
Abnormal regulation of androgen forming enzyme (P450 C17) is thought to be responsible for excess production of androgens from ovaries and adrenals.
Ovary – excess production of androgen due to
- Stimulation of theca cells by high LH,
- Enzyme hyperfunction,
- Stimulation of the cells by IGF- 1(insulin growth factor 1)
Adrenal – Excess production of androgen due to
- Enzyme hyperfunction (P450 C17)
- Stress
- High Prolactin level
Systemic Metabolic Alteration
- Hyperinsulinemia
- Hyper prolactinemia
Investigations:
- Sonography – Transvaginal sonography is more useful in obese patients. Increased numbers of peripherally arranged cysts are observed.
- LH level is elevated
- LH : FSH ratio is altered
- SHBG level decreased
- Serum testosterone and DHEA – may be marginally elevated.
- Serum insulin level elevated
- Laparoscopy
Long term risk of a patient suffering from PCOS
- Endometrial Carcinoma – The risk is greater in non obese and the patients who have not taken the OCPs. In chronic anovulatory patients with PCOS, persistently elevated estrogen levels uninterrupted by progesterone increase the risk.
- Ovarian carcinoma
- Carcinoma of breast
- Diabetes mellitus
- Hypertension and cardiovascular diseases due to abnormal lipid profile.
The PCOS Case
A patient named Dipali Majumdar, aged about 27years, unmarried female, assistant of an old allopathic physician, had been suffering from irregular and painful menstruation and diagnosed as a case of bilateral polycystic ovarian disease. At first the lady consulted with the physicians of the modern school of medicine but without getting any satisfactory result. She was advised by the old physician to consult with a homoeopath, wherein she came to me for consultation. The short description of her case is as follows:
PRESENT COMPLAINTS – Irregular, painful menstruation for last 3 years, character of blood being clotted, blackish and scanty in amount.
- No significant past history.
- Strong sycotic family history.
HOMOEOPATHIC GENERALITIES –
-
-
- Physical constitution – short but stout with dark complexion.
- Chilly patient; general aggravation in winter.
- Appetite – good.
- Desire for egg, fish, extra salt, salted food++.
- Intolerance to onion++.
- Moderate thirst for large quantities at long intervals.
- Stool hard, occasionally with mucus.
- Urine clear at regular intervals.
- Sleep sound.
- Dreams of dead persons (especially of her dead father), falling from a height++.
- Tongue – large, flabby and moist with little whitish coating & imprint of teeth.
- Palm – warm & moist.
- Teeth have irregular alignment.
- Mind – Co-operative but suspicious.
-
Dull weak memory, cannot narrate her problem properly.
INVESTIGATIONS
02/07/2001 – USG of Pelvis – Multiple cysts in both ovaries.
(Sonologist – Dr. Lipika Sen, MBBS, DMRD)
01/04/2002 – Blood report
Hb – 11.6 mg%, WBC – 7900/cumm
Neutrophil – 65%, Lymphocyte – 29%
Monocyte – 01%, Eosinophil – 05%, Basophil – 0% ESR – 48mm (1st hour)
[Pathologist – Dr. S.K.Bhattacharyya, MD (Path)]
02/04/2004 – T3 – 98ng/dl
T4 – 6.42mcg/dl
TSH – 5.49uIU/ml
[Pathologist – Dr. K.N.Sirkhell, MD (Path)]
DIAGNOSIS – Bilateral polycystic ovaries.
CHARACTERISTIC TOTALITY –
Mental generals –
-
-
- Mentally dull
- Weak memory, with difficulty in expressing her troubles
- Suspicious
-
Physical generals –
- Dreams of falling from height
- Dreams of dead persons
- Dreams of dead father
- Chilly patient
- Aggravation from onion
- Craving for salty food
Particular Symptoms –
- Painful menstruation
- Character of the menstrual blood – clotted, black.
RUBRICS TAKEN FOR REPERTORISATION
- MIND, DULLNESS, SLUGGISNESS, difficulty in thinking and comprehending
- MIND, SUSPICIOUS
- MIND, MEMORY; Weakness of, expressing oneself, for
- SLEEP, DREAMS, Dead relatives
- SLEEP, DREAMS, Dead of the
- SLEEP, DREAMS, Falling from high places
- GENERALITIES, WINTER in
- GENERALITIES, FOOD, onions agg.
- STOMACH, DESIRES, salt things
- GENITALIA FEMALE, MENSES, painful, Dysmenorrhoea
RESULT OF REPERTORISATION
- Lycopodium and Phosphorus scored highest & got 15 each, covering the seven symptoms out of ten symptoms.
- Thuja got 13 marks and covered the eight symptoms out of ten symptoms.
COMMENTS
- Lycopodium and Phosphorus scored highest & got 15 each, but Thuja covered eight symptoms out of ten. After consulting Materia medica, Thuja is preferred to be prescribed first. The typical sycotic background, sycotic constitution, chilliness of the patient etc weighed more heavily in prescribing Thuja.
PRESCRIPTIONS
12/06/2002 – Thuja occidentalis 30 / 4 doses OD
Patient was advised to come after 45 days.
First two months there was no improvement, but in general there was no aggravation and patient was in good condition. Her appetite, sleep and thirst were all normal.
After two months the painful menstruation was less severe than it was in the past. The general feeling of the patient was much better. The character of the blood was also changed from black to reddish and there was no clot (in the last menstruation).
After the first prescription only placebo was prescribed in different form from time to time.
On 10/01/2003 the menstruation became again painful with little clots with the flow, but the general feeling of the patient was better. Thuja 200 / 1 dose was prescribed.
Since then, for four months placebo was given and the patient was totally symptom free. The menstruation was regular in time, the character of the blood was red with no clot, no pain during menstruation.
Ultrasonography done on 10/05/2003, and study of uterus & ovaries appeared within normal limits with no evidence of SOL in uterus nor any cyst seen at ovaries. [ Dr K N Chakraborty, MD(Path) was the sonologist]
Since then till today patient is better and there is are no complaints of irregular or painful menstruation.
Homoeopathic Understanding of PCOS
“It is possible to find in the Organon the highest wisdom and greatest foolishness according to the natural tendency of the reader.” – August Bier.
I can’t refrain from using the very famous quotation of August Bier in writing about the homoeopathic perception of PCOS.
APHORISM – 80
….the psora, the only real fundamental cause and producer of all other numerous, I may say innumerable forms of disease that are not due to syphilis and sycosis ..under the names of nervous debility, hysteria, epilepsy and convulsions of all sorts
…..softening of the bones, scoliosis and cyphosis, caries, cancer, fungus haematodes, neoplasms, gout, haemorrhoids, haemorrhage from stomach, nose, lungs, bladder and womb, of asthma and ulceration of the lungs,.deafness, cataract, Urinary calculus, paralysis……
APHORISM NO – 205
The homoeopathic physician never treats one of these primary symptoms of chronic miasms by local remedies. The homoeopathic physician never treats one of their secondary affections that result from their further development by local remedies.
FOOT NOTE(205)- EXAMPLE
If this dynamic remedy should indeed succeed in freeing the affected part of the body from the malignant ulcer locally, the basic malady is thereby not diminished in the slightest,
…….the preserving vital force is therefore necessitated to transfer the field of operation of the great internal malady to some more important part (as it does in every case of metaschematism)
FOOT NOTE(205)
Without previous cure of the inner miasm (6th ed) when cancer of the face or breast is removed by the knife alone ….something worse ensues, or at any rate death is hastened. But the old school still goes blindly on in the same way in every new case, with the same disastrous results.
So, from these important quotations it is quite evident that we should not bother with the nosological diagnosis only. The cause is to be searched out by keen observations and exhaustive case taking. The clues may remain in the family history, past history, or in the individual’s individuality (caharacteristics), socio – cultural – environmental field etc. and then only can it be claimed as true anamnesis of the case. The concept of local maladies and the surgical removal of it are the basic misunderstanding of the disease that prevails in the medical field. The patient’s high susceptibility to the disease or the miasmatic tendencies of the patient in favour of formation of PCOS, or severe insult found in the anamnesis which has hurt the individual, or the continuous stress with tension /grief / mortification / reserved displeasure or even the iatrogenic factor and in a few cases some mechanical factor for prolonged periods are the real causes to be investigated to reach to the similimum. The following points are to be remembered:
- The disease cannot be considered as local without considering the whole – the basic philosophy of homoeopathy
- Even if the remedy is given dynamically to the patient, if it only addresses the disease locally, without considering the whole – then we are treating wrongly.
- Surgical removal cannot cure the inner disease.
- Without curing the inner miasms with the suitable simillimum, any type of external application or surgical removal are futile efforts.
- To cure a chronic disease, the physician has to go to the depth of the disease with his unique case taking processes which will ultimately individualize the case.
- To know the fundamental cause one should have a clear conception of miasms according to the master Samuel Hahnemann.
- To know the miasm one should have sound knowledge of the symptomatology of the three different miasms.
- The deeper understanding of miasms and their symptomatology cannot only be ascertained theoretically from our masters, but must be perceived in clinical practice by keen observation.
- The mechanical attitude to the disease still prevails, though modern medicine makes some pretense to be holistic. It still differs from the homoeopathic concept of holism.
The disease cannot be under the domain of any one miasm. In the pathophysiology part of the disease , the real cause is yet to be known and few hypotheses are made. We cannot forget Psora in this disease, because in all of the hypotheses the basic factors remain in the irregularities of the function of the endocrine system. The excessive discharge or the lesser discharge are factors which are created due to the functional abnormalities. The pathophysiology and the symptomatology differ in each patient. From the homoeopathic viewpoint, it is not the disease that determines its manifestation, but rather the individual’s character, miasmatic back ground, hereditary influences, environmental factors etc. which predetermine the form of manifestation in an individual.
It is quite evident that all the symptomatology under the PCOS cannot be manifested in each patient and now it is clearly understood that the patient with sycotic predominance will present the sycotic symptology of the disease, and the syphilitic predominant patient presents with the syphilitic features and so on. In case of mixed miasmatic background (which is common to all cases nowadays) the feature of that miasm which is most prominent at the time can be seen in conjunction with the symptoms of other miasms in less intense form.
In taking the case of PCOS, the emphasis should be given to the medical history, iatrogenic history, marital and obstetrical history, sexual history, social history. The mental and physical makeup of the patient should be observed with utmost scrutiny.
In my clinical practice I have got good results, but have failed also and those failed cases showed me the way to perceive disease in the true sense. I have put this particular case before you, because it is well documented.


Hi,
I read your whole article, made a lot of sense. Thank you for sharing.
Hi Rajat,
Take my salam, hope u r fine n good health.
I read u article, it is good, it’s help the Homoeopath.
Thanking you,
Prof Dr S S Rahman, Dubai, UAE.
hi, its nice artical. Even my self I have used the same medicine for overian cyct treatment. thanks
brilliant! the humility and honesty of the practitioner is worth emulating!
These experiments makes the sure and proud to the Homeopathy & to Homeopath.Thank you very much for the artcle
Sir,
I have read this article,which is giving the way to the treatment of incurable disease of PCOS. I find it is very good article. I want also to contact about a case of multiple ovarian cyst with uterine fibroid.
Thanks and waiting for reply.
Hi, I read this case, I want to know if her hirsutism was also solved.I have severe hirsutism and I am desperate.If one perosn was cured, there’s still hope. I’m seeing a homeopath and taking what he’s prescribing, but I see no change.
These experiments makes the sure and proud to the Homeopathy & to Homeopath.Thank you very much for the article
EXCELLENT ARTICLE KEEP IT UP.
regards
Dr. Raaj
Excellent, please go ahead with more cases.
Hi sir.. i am very much impressed with ur article.. hirsutism is really curable in homeo???
great article!!! I want to know about hirsutism, is it resolved???
Dear Doctor,
My wife aged 34 is suffering from Ovarian Cyst ( on right ovary about 4 CM in size) and PCOD on left ovary.
She had this (Endometriosis with Ovarian Cyst) problem earlier also, then we had to go for IVF during first pregnancy.
Now after delivery (4 months after delivery) again this problem has been detected.
As in allopathy only surgery is the option to remove cyst and it is difficult to conceive with cyst on ovary.
Please help us.
If you require latest TVS (sonography) report i’ll send you. Please provide your Email ID.
Congratulations to all your efforts,
may God help you continue your efforts efficiently, prayings.