


Key words: Foot, Trophic, Non-healing, Homoeopathy, Nitric Acid.
Introduction:
Abstract: A case study of chronic non-healing trophic foot ulcer in a 24- year-old woman treated with homoeopathy based on her totality of symptoms. The ulcer was healed in a very short time with the selected simillimum.
The word ‘Trophic’ is derived from the Greek word Trophe meaning ‘nutrition’. Merriam-Webster.com Medical Dictionary defines trophic ulcer as ‘an ulcer (as bedsore) caused by faulty nutrition in the affected part’. Mosby’s Medical Dictionary 2009 defines trophic ulcer as ‘a pressure ulcer caused by external trauma to a part of the body that is in poor condition because of disease, vascular insufficiency or loss of afferent nerve fibres’.
Trophic ulcers can be classified as tabulated in below table:
Classification of Trophic ulcer1:
| S.no | Types: | Disease states: |
| 1 | Neurogenic | E.g.: Syringomyelia, Spina bifida, Neuropathy, Leprosy. |
| 2 | Vascular (arterial) | Angiopathy in Diabetics, other poor Arterial supply diseases like Arteriosclerosis. |
| 3 | Vascular (venous) | Venous stasis ulcers. |
| 4 | Systemic causes | Malnutrition, Vitamin B12 deficiency. |
Fig: 01 TROPHIC ULCER

NEUROGENIC ULCERS2: The mechanism of formation of such ulcer is repeated injury or pressure in an area which has lost appreciation of pain. Neurogenic/Neuropathic ulcers (Figure: 01) on the soles of the feet or fingertips usually develop at sites exposed to repeated high pressures during daily activities like walking or standing for long hours.
These ulcers are commonly seen on the heel and ball of the foot when the patient is ambulatory; on the buttock and on the back of the heel when the patient is non-ambulatory. This ulcer starts with callosity under which suppuration takes place.
The pus comes out and the central hole forms the ulcer which gradually burrows through the muscles and the tendons to the bone. That is why this ulcer is also called perforating ulcer. These ulcers are painless. People with normal sensation in their extremities can do avoidance measures like changing gait or modifying activity.
However, in patients with peripheral sensory deficits as in spina bifida/ neuropathy cases, where pain perception is absent, they do not relieve pressures. Hence, the repetitive trauma leads to skin breakdown and ulceration.
The neurological conditions which predispose to the formation of such ulcer include diabetes, alcoholic peripheral neuritis, Tabes dorsalis, spina bifida (e.g. Meningomyelocele), leprosy, peripheral nerve injury, paraplegia and Syringomyelia.
A detailed history and clinical examination will help diagnose and classify the ulcer as diabetic, venous, arterial, neuropathic, pressure sore or due to malnutrition.
MENINGOMYELOCELE3: A type of Spina bifida, where the normally developed spinal cord or cauda equina is protruded along with the meninges and these structures may be adherent to the posterior aspect of the sac. It is the most common type of spina bifida in children.
Neurological manifestations are almost always present and there may be sensory disturbances along with trophic changes in the lower extremities. Trophic Ulcers are very common in pressure areas. There may be motor disturbances and in advanced cases, one may find extensive paralysis of the legs. Urinary incontinence is also seen.
Case Study:
Presenting Illness:
A female patient of 24 years came to OPD at Government Homoeopathic Dispensary with the following complaints:
- Painless ulcer on the heel of right foot since 3 years, formed after a minor trauma when walking, which is deep with ragged edges and exposing inner muscles of foot.
- Painless Swelling around right ankle.
- No sensation in right lower limb for external pressure or any stimuli.
- Completely lost control of urination. Wears diapers every day.
Past History:
- Born with congenital spinal disease at birth. diagnosed as
Treatment History:
- She underwent surgery at three days old.
Family History:
- Mother is diabetic and suffers occasionally from seizures since her childhood for which she is using antiepileptic drugs.
- Father is apparently healthy.
Mental generals:
- She is anxious about her health and the future due to this complaint. Worried about the incurability of her complaint.
- She is dissatisfied with her life, feels isolated as she stays continuously at home due to her problem.
- Hates her parents as she feels they are responsible for her illness.
- Fear of cancer as this illness is incurable and may end in cancer of her foot.
- Avoids meeting friends and family members. Desires to be alone even though she feels isolated.
Physical Generals:
- Thirsty, Desires Sweets+, Aversion to meat, Perspiration more on the neck, Regular Bowels, Dreams not particular, sleeps for 6 hours, refreshing.
General Physical Examination:
- Fair, 5.6 Height, 65 kgs weight, moderately built.
- No signs of Pallor, Generalized Odema, Lymphadenopathy, Cyanosis, Clubbing, Icterus.
Vital signs:
B.P: 130/70 MM HG, P/R: 74/MIN, H/R: 74/MIN, R.R: 19/MIN
Systemic Examination:
- CVS: NAD
- GASTRO-INTESTINAL: NAD
- LOCOMOTOR: Mild Deformity of Right Foot. Charcot’s Joint?
- NEUROLOGICAL SYSTEM: Loss of reflexes- Negative for all reflexes in the right knee and foot joints, Sensory loss in the right gluteal region and right lower limb. Low muscle tone and strength of the right leg.
- SKIN: Ulcer on the heel of the right foot.
Ulcer: Pain: Absent, Depth: deep up to muscles, Discharge: Absent, Odor: Odorless, Edges: Ragged with dry scaly tissue, Floor: Non-healing, poor and pale granulation tissue, Slight induration of the base. Clinically callus type. Lymph nodes: Not palpable. For assessing the severity of the ulcer Meggitt -Wagner Classification of Foot ulcer4 is used. According to the classification, ulcer comes under Grade -02.

Investigations:
- CBP: Normal study, Test for Blood sugars: FBS: 98 mg/ml, PLBS: 115 mg/ml. CUE: Normal findings, NERVE CONDUCTING STUDY OF LOWER LIMBS: suggesting sensory-motor neuropathy of right lower limb.
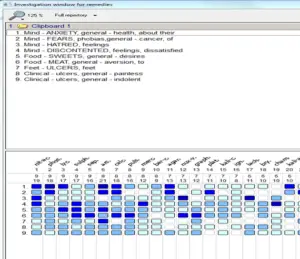
Repertorisation:
The case was repertorized in radar repertory (figure-02) with the following rubrics and the selected drug was Acid nitric 30 CH. She was given a single dose on 28/02/2022 after repertorising and advised to maintain the hygiene of ulcer.
Rubrics selected based on the following symptoms:
- Anxiety about health
- Fear of cancer
- Hatred towards parents
- Dissatisfied life
- Desires sweets
- Aversion to meat
- Ulcers of feet
- Painless ulcers
- Indolent ulcers
Fig: 02 Repertorization results.
Follow up of the case:
| DATE OF VISITING | SYMPTOMS | TREATMENT GIVEN | |
| FIRST FOLLOW-UP after 30 days : 23/03/2022 | Change in the depth of ulcer is noted. Scaly tissue in the surrounding of ulcer had decreased. | PLACEBO FOR 30 DAYS. | |
| SECOND FOLLOW UP:
26/04/2022 |
Signs of healing (Fig: 03) are seen. Ulcer depth was mostly covered by new tissue. No scaly tissue seen. Edges of ulcer are not seen properly. (Fig: 03)
|
PLACEBO FOR 30 DAYS | |
| THIRD FOLLOW UP:
04/05/2022 |
Ulcer healed to the maximum. New scar tissue is noted on the top of it.
|
One Dose of Acid Nitric 30 repeated to hasten the healing. SL for 4 Weeks. | |
| FOURTH FOLLOW UP:
02/06/2022 |
Signs of ulcer got completely lost on the foot. (Fig:05)
|
Given PLACEBO for three weeks. |



Results and discussion:
This case of stubborn chronic non-healing trophic ulcer of Grade 02, according to Meggitt-Wagner Classification of Foot ulcer, didn’t respond to any sort of conventional treatment and other surgical procedures. However, post homoeopathic treatment, the ulcer was almost healed.
The patient is advised be careful of being injured since the chances of new ulcers are inevitable in this case due to lost sensation in her leg. She was advised to take necessary oral supplements like Vitamin B12 and other nutraceuticals to prevent neuropathy. She was advised to continue homoeopathic medicines if any illness noted in the foot.
Acknowledgement:
I sincerely express my gratitude to Dr. V.S. Alagu Varshini, I.A.S, Director, Department of AYUSH, Telangana State, and Dr. Ravi Naik, Regional Deputy Director, Department of Ayush, Telangana State for encouraging us in the dispensaries to treat the patients. My sincere thanks to the patient’s family for their consent to use homoeopathic treatment and for having faith in homoeopathy. Last but not least, I must acknowledge Dr. Samuel Hahnemann, the father of homoeopathy, for discovering this science for humanity. AUDE SAPERE.
REFERENCES:
- Ghauri AS, Nyamekye IK. Leg ulceration: The importance of treating the underlying pathophysiology. Phlebology 2010;25 (Suppl 1):42-51.
- Somen Das, A concise textbook of Surgery, Sixth Edition, 2010, Ulcer, Sinus, Fistula, page: 159-160.
- Somen Das, A concise textbook of Surgery, Sixth Edition, 2010, Ulcer, Sinus, Fistula, page: 389
- https://www.researchgate.net/figure/Meggitt-Wagner-classification-of-foot-ulcers_tbl1_224821575.


Very classical treatment of homeopathy. Great that you are treating in the goverment hospital such type of cases. Spread homeopathy in the villages to gain confidence and knowledge in the people. Many people doesn’t know about the system of homeopathic treatment and gentle way of healing..